

A 24-week multicentre, randomized, open-label, parallel-group study comparing the efficacy and safety of ixekizumab vs. fumaric acid esters and methotrexate in patients with moderate-to-severe plaque psoriasis naive to systemic treatment
- PMID: 31376153
- PMCID: PMC7187169
- DOI: 10.1111/bjd.18384
A 24-week multicentre, randomized, open-label, parallel-group study comparing the efficacy and safety of ixekizumab vs. fumaric acid esters and methotrexate in patients with moderate-to-severe plaque psoriasis naive to systemic treatment
Abstract
Background: Interleukin-17 antagonists have received a first-line label for moderate-to-severe plaque psoriasis.
Objectives: We conducted the first head-to-head trial between the two most commonly used first-line therapies in Germany, fumaric acid esters (FAEs) and methotrexate, and the interleukin-17A antagonist, ixekizumab.
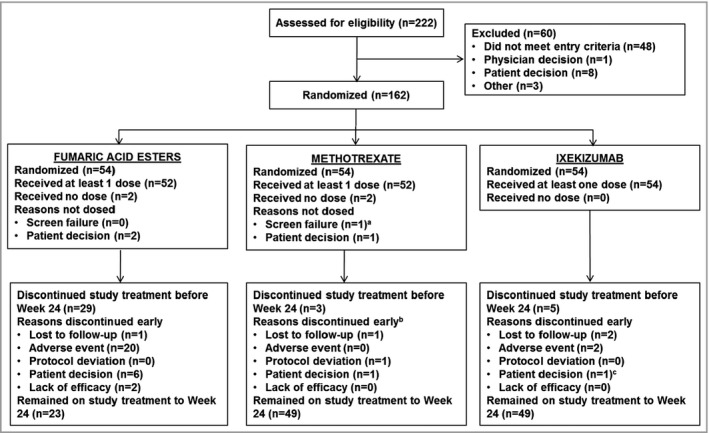
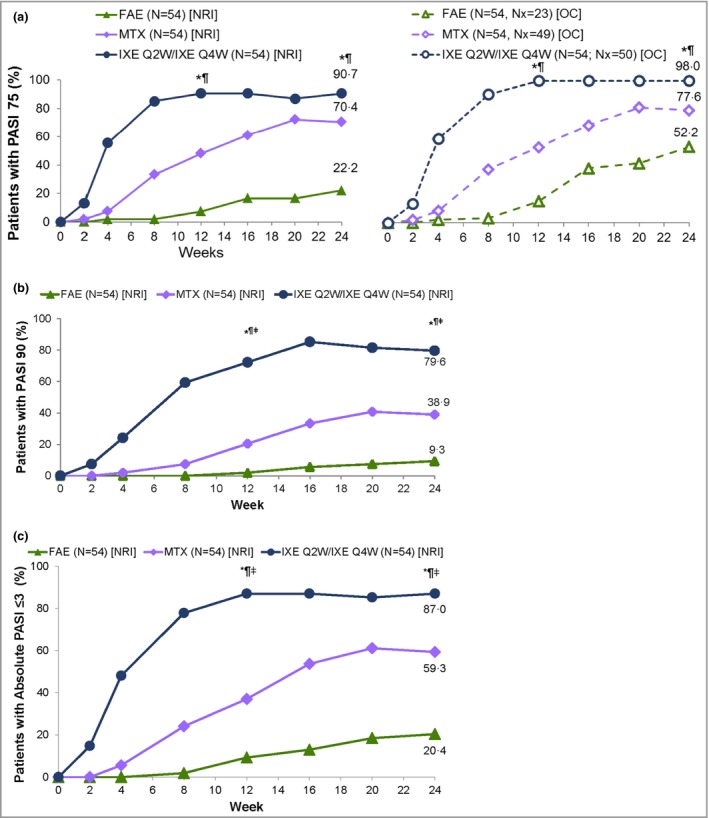
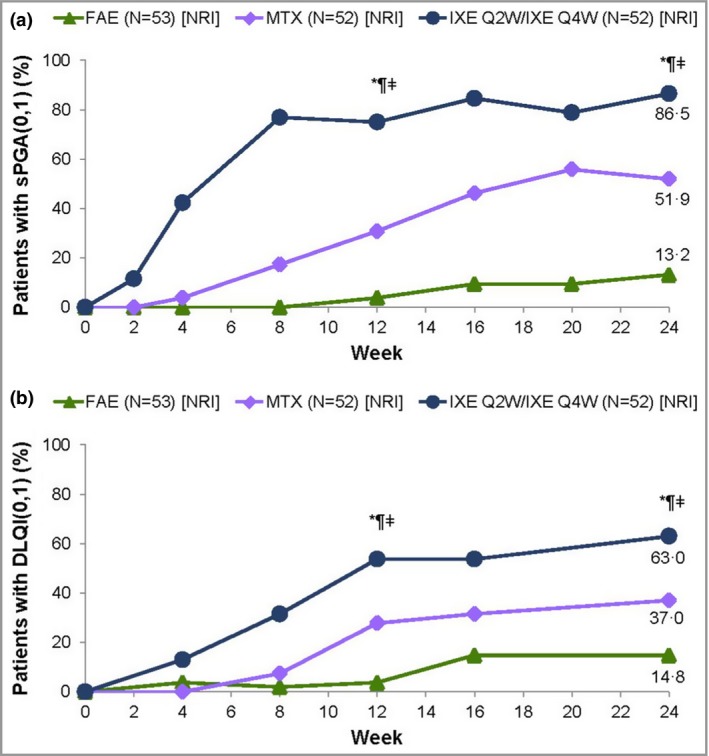
Methods: Systemic-naive patients were randomized in this parallel-group, active-comparator, open-label, rater-blinded trial (each group n = 54). The primary outcome was the proportion of patients achieving ≥ 75% improvement in Psoriasis Area and Severity Index (PASI 75) at 24 weeks. Key secondary outcomes included 24-week PASI 90 and 100, static Physician's Global Assessment (sPGA) score of 0 or 1, and Dermatology Life Quality Index (DLQI) score of 0 or 1. Safety events at week 24 were analysed using Fisher's exact test. Missing data were imputed using nonresponder imputation. The trial was registered at ClinicalTrials.gov (NCT02634801) and EudraCT (2015-002649-69).
Results: At week 24, more ixekizumab-treated patients achieved PASI 75 [91% vs. 22% FAEs (P < 0·001) and 70% methotrexate (P = 0·014)], PASI 90 [80% vs. 9% FAEs (P < 0·001) and 39% methotrexate (P < 0·001)] and PASI 100 [41% vs. 4% FAEs (P < 0·001) and 13% methotrexate (P = 0·0041)], as well as sPGA (0,1) and DLQI (0,1).
Conclusions: Ixekizumab was superior in inducing PASI 75/90/100, sPGA (0,1) and DLQI (0,1) responses at week 24 compared with methotrexate and FAEs. Safety profiles for all treatments were consistent with prior studies.
© 2019 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Figures
References
-
- Nast A, Boehncke WH, Mrowietz U et al German S3‐guidelines on the treatment of psoriasis vulgaris (short version). Arch Dermatol Res 2012; 304:87–113. - PubMed
-
- Saurat JH, Stingl G, Dubertret L et al Efficacy and safety results from the randomized controlled comparative study of adalimumab vs. methotrexate vs. placebo in patients with psoriasis (CHAMPION). Br J Dermatol 2008; 158:558–66. - PubMed
-
- Barker J, Hoffmann M, Wozel G et al Efficacy and safety of infliximab vs. methotrexate in patients with moderate‐to‐severe plaque psoriasis: results of an open‐label, active‐controlled, randomized trial (RESTORE1). Br J Dermatol 2011; 165:1109–17. - PubMed
-
- Cosentyx® (secukinumab). Summary of product characteristics. Available at: https://ec.europa.eu/health/documents/community-register/2015/2015011513... (last accessed 22 August 2019).
-
- Taltz® (ixekizumab). [Summary of product characteristics]. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Info... (last accessed 22 August 2019).
