

Impact of implementation of an enhanced recovery program in gynecologic surgery on healthcare costs
- PMID: 31376395
- PMCID: PMC7123521
- DOI: 10.1016/j.ajog.2019.07.039
Impact of implementation of an enhanced recovery program in gynecologic surgery on healthcare costs
Abstract
Background: Enhanced recovery programs have been associated with improved outcomes after gynecologic surgery. There are limited data on the effect of enhanced recovery programs on healthcare costs or healthcare service use.
Objective: The purpose of this study was to evaluate differences in hospital charges for women who undergo surgery for a suspected gynecologic cancer that is managed in an enhanced recovery program as compared with conventional perioperative care.
Study design: We performed a retrospective cohort study of women who underwent open abdominal surgery for a suspected gynecologic cancer before and after the implementation of an enhanced recovery after surgery program. Consecutive patients from May to October 2014 and from November 2014 to November 2015 comprised the conventional perioperative care (before enhanced recovery after surgery) and enhanced recovery after surgery cohorts, respectively. Patients were excluded if they underwent surgery with a multidisciplinary surgical team or minimally invasive surgery. All technical and professional charges were ascertained for all healthcare services from the day of surgery until postoperative day 30. Charges for adjuvant treatment were excluded. Charges were classified according to the type of clinical service provided. The primary outcome was the difference in total hospital charges between the pre-enhanced recovery after surgery and the enhanced recovery after surgery groups. Secondary outcomes were between group differences in hospital charges within clinical service categories.
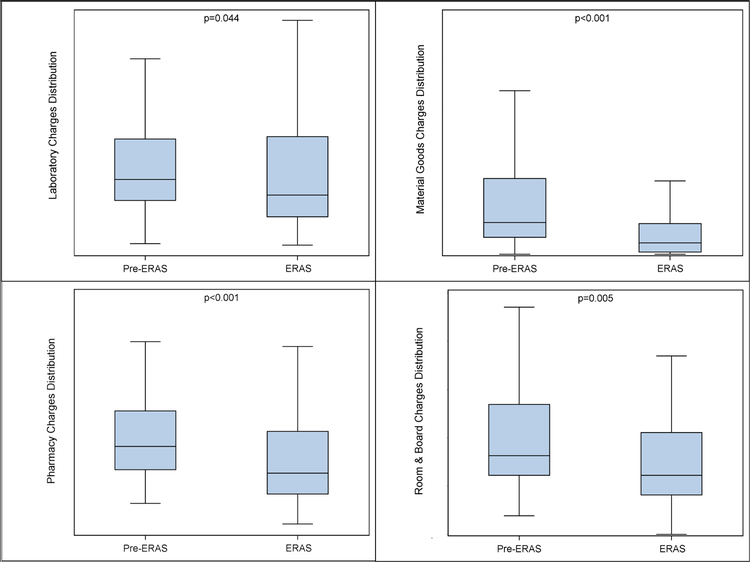
Results: A total of 271 patients were included in the analysis (58 patients in the pre-enhanced recovery after surgery and 213 patients in the enhanced recovery after surgery cohort). A total of 70,177 technical charges and 6775 professional charges were identified and classified. The median hospital charge for a patient decreased 15.6% in the enhanced recovery after surgery group compared with the pre-enhanced recovery after surgery group (95% confidence interval, 5-24.5%; P=.008). Patients in the enhanced recovery after surgery group also had lower charges for laboratory services (20% lower; 95% confidence interval, 0--39%; P=.04), pharmacy services (30% lower; 95% confidence interval, 14--41%; P<.001), room and board (25% lower; 95% confidence interval, 20--47%; P=.005), and material goods (64% lower; 95% confidence interval, 44--81%; P<.001). No differences in charges were observed for perioperative services, diagnostic procedures, emergency department care, transfusion-related services, interventional radiology procedures, physical/occupational therapy, outpatient care, or other services.
Conclusion: Hospital charges and healthcare service use were lower for enhanced recovery patients compared with patients who received conventional perioperative care after open surgery for a suspected gynecologic cancer. Enhanced recovery programs may be considered to be high value in healthcare because they provide improved outcomes while lowering resource use.
Keywords: enhanced recovery after surgery; gynecologic surgery; postoperative care.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
DISCLOSURES:
The authors report no conflicts of interest, financial or otherwise, related to the subject matter of the article submitted.
Figures

References
-
- Nelson G, Altman AD, Nick A, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS(R)) Society recommendations--Part I. Gynecol Oncol. 2016;140(2):313–322. - PubMed
-
- Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017;152(3):292–298. - PubMed
-
- de Groot JJ, Ament SM, Maessen JM, Dejong CH, Kleijnen JM, Slangen BF. Enhanced recovery pathways in abdominal gynecologic surgery: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2016;95(4):382–395. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
