

Stereotactic Ablative Radiation Therapy (SAbR) Used to Defer Systemic Therapy in Oligometastatic Renal Cell Cancer
- PMID: 31377159
- PMCID: PMC7647381
- DOI: 10.1016/j.ijrobp.2019.07.023
Stereotactic Ablative Radiation Therapy (SAbR) Used to Defer Systemic Therapy in Oligometastatic Renal Cell Cancer
Abstract
Purpose: Stereotactic ablative radiotherapy (SAbR) is a promising alternative for selected patients with renal cell carcinoma (RCC) with oligometastasis. The objective of this study was to evaluate the potential of SAbR for longitudinal control in patients with persistently oligometastatic RCC. We report the impact of SAbR on tumor control rates as well as its tolerability in systemic therapy-naïve patients with oligometastatic disease (without brain metastases) and assess the effect of SAbR on subsequent first line systemic therapy by comparison to historical controls.
Methods and materials: We reviewed patients with metastatic RCC treated with front-line SAbR with a curative intent from 2007 to 2017 at UT Southwestern Kidney Cancer Program. We analyzed local control rates (LCR), toxicity, freedom from systemic therapy (FST), type and duration of first-line systemic therapy, and overall survival (OS). Cox regression and Kaplan-Meier analyses were used.
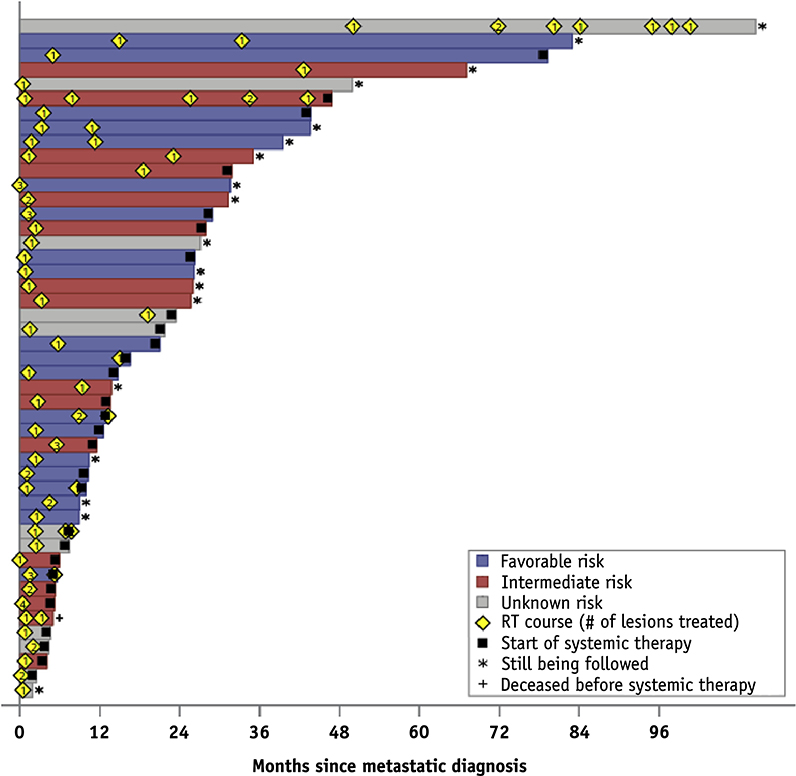
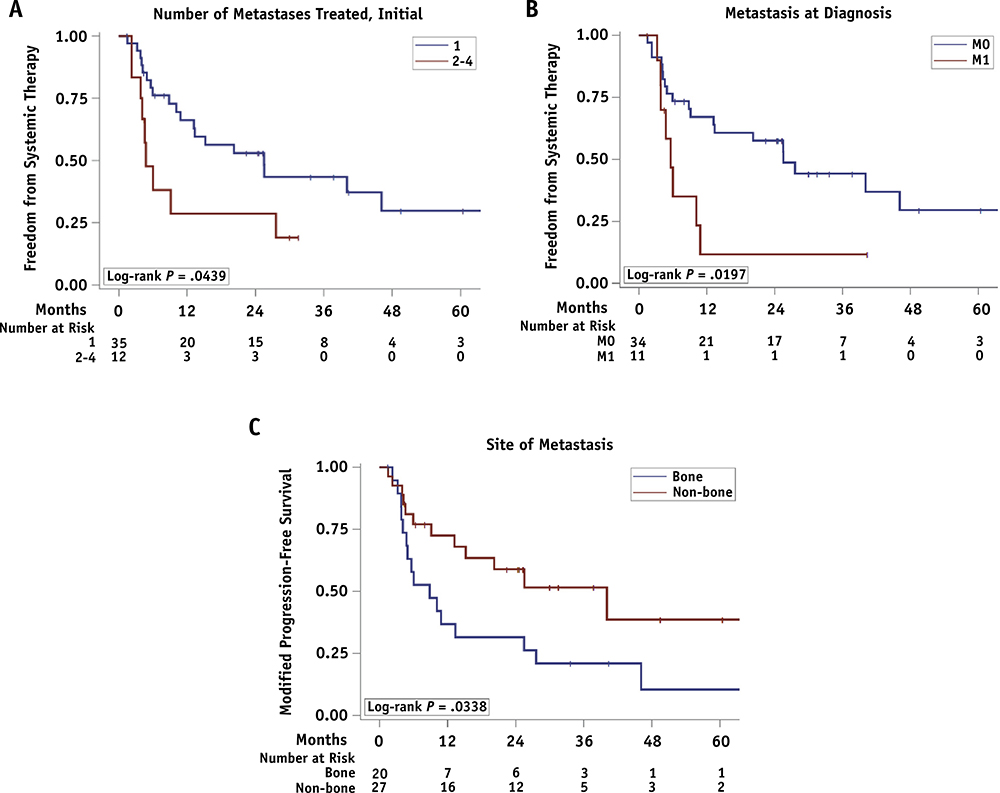
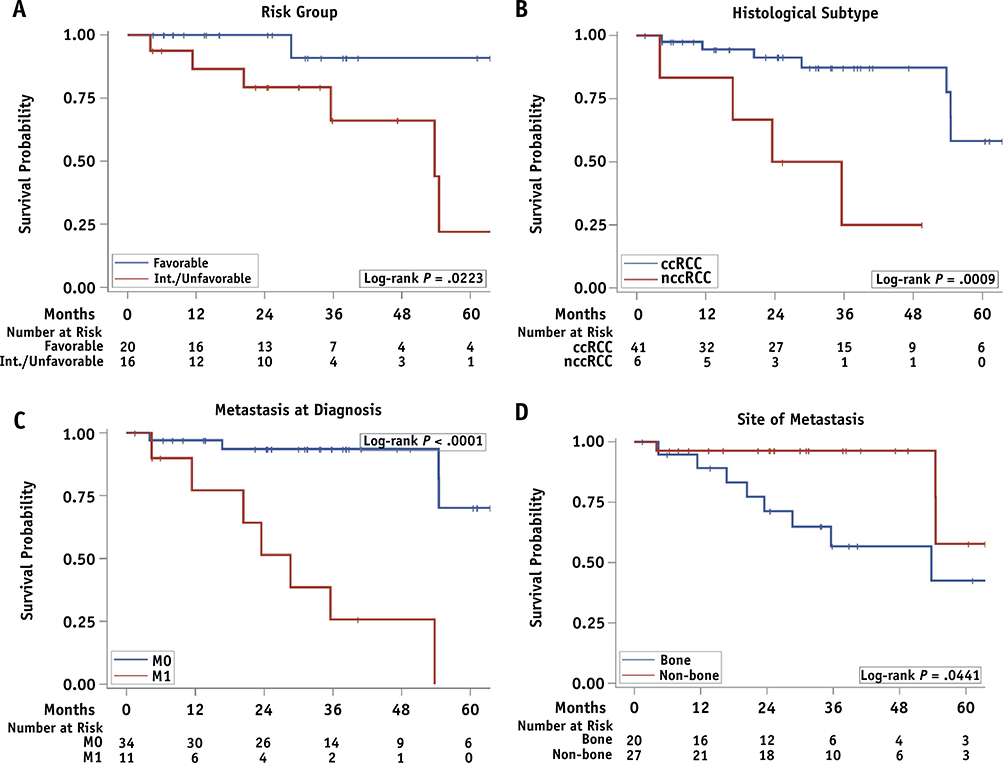
Results: We identified 47 patients with oligometastatic RCC treated with SAbR to 88 metastases; 11 patients had more than 1 SAbR course. The local control rate was 91.5% at 2 years with no reported grade ≥3 toxicity. With a median follow-up of 30 months (interquartile range, 13.7-40.9), median FST from first SAbR was 15.2 months (95% confidence interval [CI], 8.8-40.1). The most common systemic therapies initiated after SAbR were pazopanib (60.7%) and sunitinib (14.3%). The duration of first line systemic therapy appeared unaffected by SAbR. Improved FST was observed in patients with metachronous disease (hazard ratio, 2.67; P = .02), solitary metastasis (HR, 2.26; P = .05), and non-bone metastasis (HR, 2.21; P = .04). One-year and 2-year OS after SAbR were 93.1% (95% CI, 80.1-97.7) and 84.8% (95% CI, 69.1-92.9), respectively. Median OS was not reached.
Conclusions: SAbR is an effective and safe treatment for selected patients with oligometastatic RCC, can provide longitudinal disease control without systemic therapy for over a year, and does not appear to adversely affect the effectiveness of first-line systemic therapy once initiated. Prospective validation of these findings is being sought through a phase 2 trial.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Znaor A, Lortet-Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur Urol 2015;67:519–530. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66:7–30. - PubMed
-
- Rabinovitch RA, Zelefsky MJ, Gaynor JJ, Fuks Z. Patterns of failure following surgical resection of renal cell carcinoma: Implications for adjuvant local and systemic therapy. J Clin Oncol 1994;12:206–212. - PubMed
-
- Kim SP, Weight CJ, Leibovich BC, et al. Outcomes and clinicopathologic variables associated with late recurrence after nephrectomy for localized renal cell carcinoma. Urology 2011;78:1101–1106. - PubMed
-
- Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol 1995; 13:8–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
