

Initiation of sodium polystyrene sulphonate and the risk of gastrointestinal adverse events in advanced chronic kidney disease: a nationwide study
- PMID: 31377791
- PMCID: PMC7473802
- DOI: 10.1093/ndt/gfz150
Initiation of sodium polystyrene sulphonate and the risk of gastrointestinal adverse events in advanced chronic kidney disease: a nationwide study
Abstract
Background: Despite long-standing clinical use of sodium polystyrene sulphonate (SPS) for hyperkalaemia management in chronic kidney disease (CKD), its safety profile remains poorly investigated.
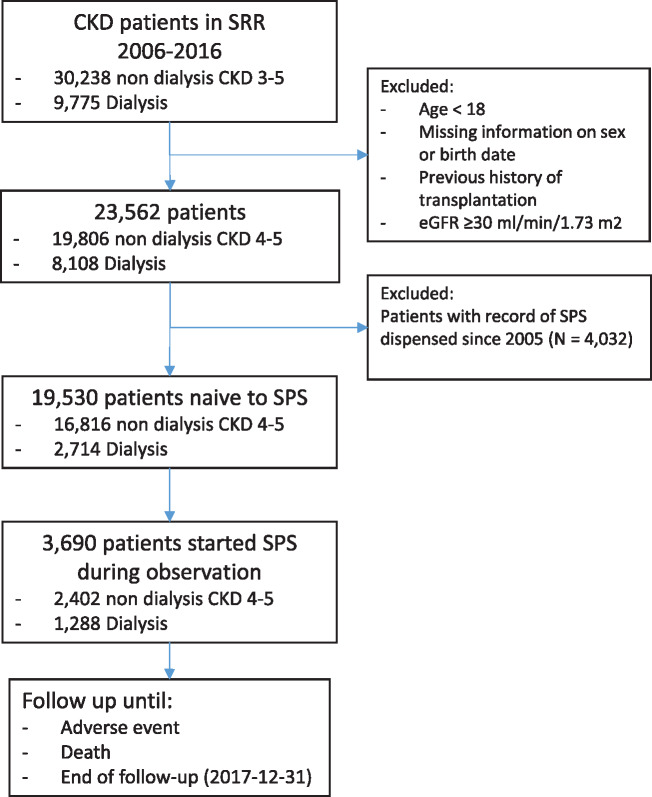
Methods: We undertook an observational analysis of nephrology-referred adults with incident CKD Stage 4+ in Sweden during 2006-16 and with no previous SPS use. We studied patterns of use and adverse events associated to SPS initiation during follow-up. Patterns of SPS use were defined by chronicity of treatment and by prescribed dose. We estimated hazard ratios (HRs) and 95% confidence intervals (CIs) associated with SPS initiation (time-varying exposure) for the risk of severe (intestinal ischaemia, thrombosis or ulceration/perforation) and minor (de novo dispensation of laxatives or anti-diarrheal drugs) gastrointestinal (GI) events.
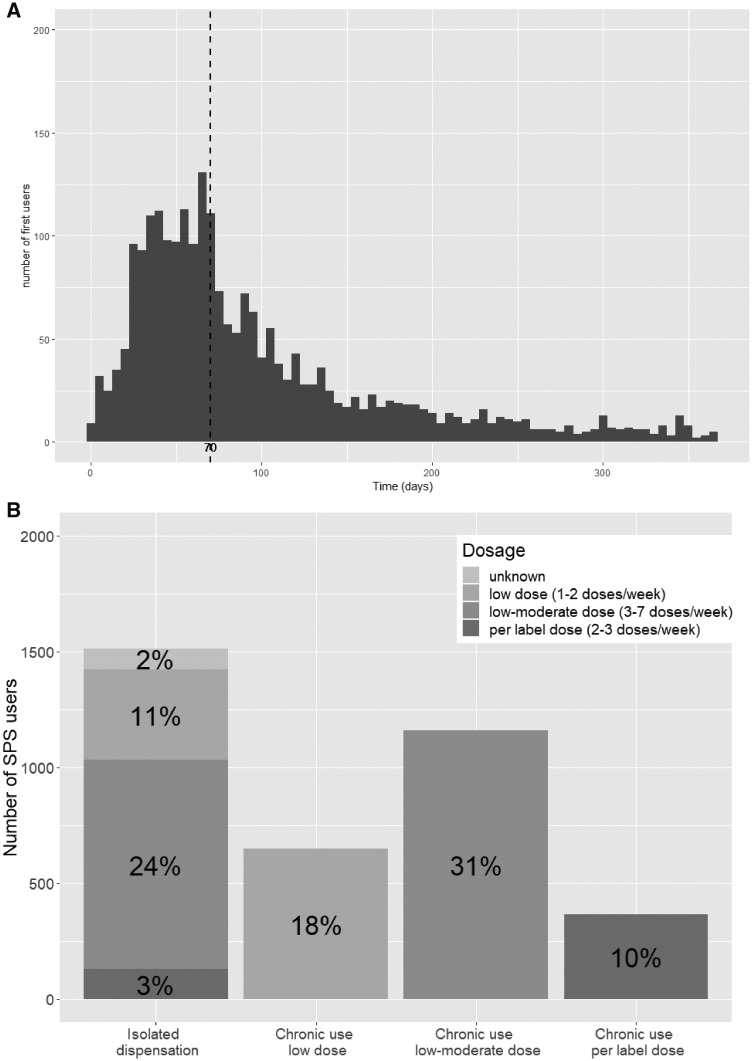
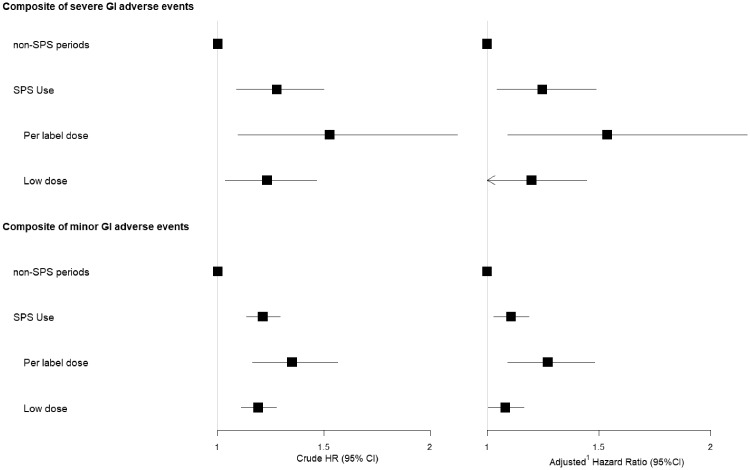
Results: Of 19 530 SPS-naïve patients with CKD, 3690 initiated SPS during follow-up. A total of 59% took SPS chronically, with an average of three dispensations/year. The majority (85%) were prescribed lower dosages than specified on the product label. During follow-up, 202 severe and 1149 minor GI events were recorded. SPS initiation was associated with a higher incidence of severe adverse events [adjusted HR 1.25 95% CI 1.05-1.49)], particularly in those receiving per label doses [1.54 (1.09-2.17)] and mainly attributed to ulcers and perforations. SPS initiation was also associated with higher incidence of minor GI events [adjusted HR 1.11 (95% CI 1.03-1.19)], regardless of dose, and mainly accounted for by de novo dispensation of laxatives.
Conclusions: Initiation of SPS in patients with advanced CKD is associated with a higher risk of severe GI complications as well as the initiation of GI-related medications, particularly when prescribed at per label doses.
Keywords: CKD; chronic haemodialysis; chronic renal failure; epidemiology; hyperkalaemia.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
Comment in
-
Sodium polystyrene sulfonate: still news after 60 years on the market.Nephrol Dial Transplant. 2020 Sep 1;35(9):1455-1458. doi: 10.1093/ndt/gfaa004. Nephrol Dial Transplant. 2020. PMID: 32040164 No abstract available.
References
-
- Nilsson E, Gasparini A, Arnlov J. et al. Incidence and determinants of hyperkalemia and hypokalemia in a large healthcare system. Int J Cardiol 2017; 245: 277–284 - PubMed
-
- Kovesdy CP, Appel LJ, Grams ME. et al. Potassium homeostasis in health and disease: a scientific workshop cosponsored by the National Kidney Foundation and the American Society of Hypertension. Am J Kidney Dis 2017; 70: 844–858 - PubMed
-
- Sterns RH, Rojas M, Bernstein P. et al. Ion-exchange resins for the treatment of hyperkalemia: are they safe and effective? J Am Soc Nephrol 2010; 21: 733–735 - PubMed
