

Dual CCR5/CCR2 targeting: opportunities for the cure of complex disorders
- PMID: 31377844
- PMCID: PMC6892368
- DOI: 10.1007/s00018-019-03255-6
Dual CCR5/CCR2 targeting: opportunities for the cure of complex disorders
Abstract
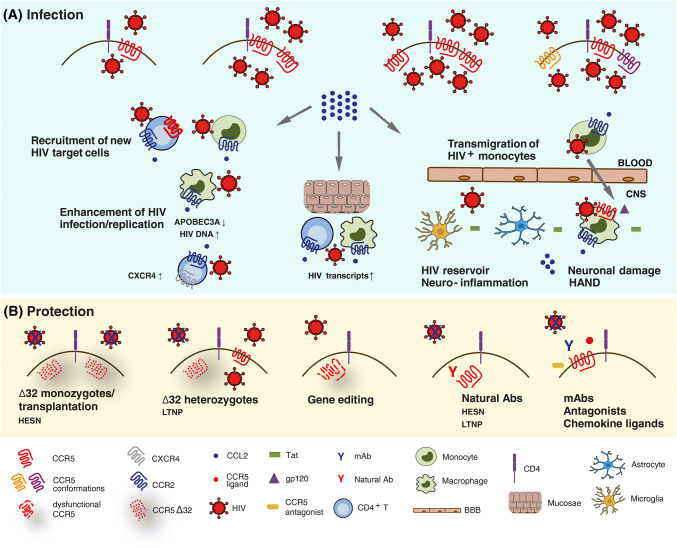
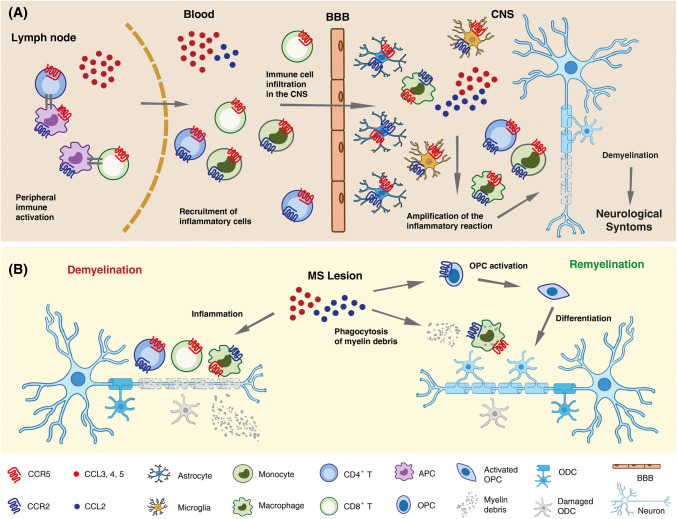
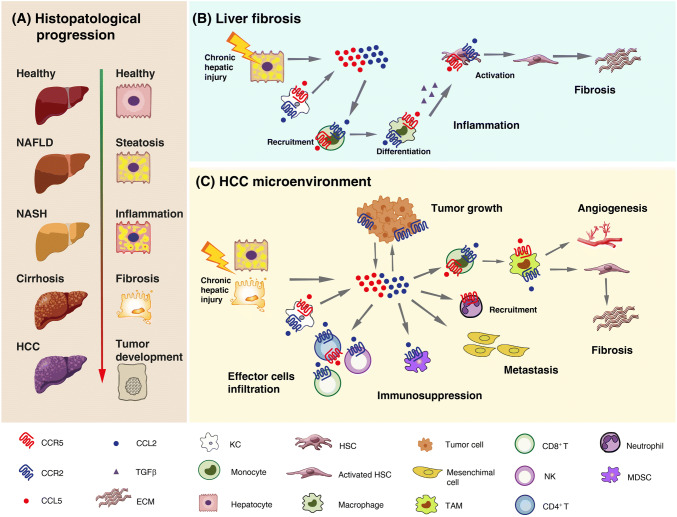
The chemokine system mediates acute inflammation by driving leukocyte migration to damaged or infected tissues. However, elevated expression of chemokines and their receptors can contribute to chronic inflammation and malignancy. Thus, great effort has been taken to target these molecules. The first hint of the druggability of the chemokine system was derived from the role of chemokine receptors in HIV infection. CCR5 and CXCR4 function as essential co-receptors for HIV entry, with the former accounting for most new HIV infections worldwide. Not by chance, an anti-CCR5 compound, maraviroc, was the first FDA-approved chemokine receptor-targeting drug. CCR5, by directing leukocytes to sites of inflammation and regulating their activation, also represents an important player in the inflammatory response. This function is shared with CCR2 and its selective ligand CCL2, which constitute the primary chemokine axis driving the recruitment of monocytes/macrophages to inflammatory sites. Both receptors are indeed involved in the pathogenesis of several immune-mediated diseases, and dual CCR5/CCR2 targeting is emerging as a more efficacious strategy than targeting either receptor alone in the treatment of complex human disorders. In this review, we focus on the distinctive and complementary contributions of CCR5 and CCR2/CCL2 in HIV infection, multiple sclerosis, liver fibrosis and associated hepatocellular carcinoma. The emerging therapeutic approaches based on the inhibition of these chemokine axes are highlighted.
Keywords: AIDS; Autoimmunity; Chemokine receptor antagonist; Liver disease; Neuroinflammation; Therapeutic antibody.
Figures
References
-
- Griffith JW, Sokol CL, Luster AD. Chemokines and chemokine receptors: positioning cells for host defense and immunity. Annu Rev Immunol. 2014;32:659–702. - PubMed
-
- Szpakowska M, Fievez V, Arumugan K, van Nuland N, Schmit JC, Chevigne A. Function, diversity and therapeutic potential of the N-terminal domain of human chemokine receptors. Biochem Pharmacol. 2012;84:1366–1380. - PubMed
-
- Lu M, Wu B. Structural studies of G protein-coupled receptors. IUBMB Life. 2016;68:894–903. - PubMed
-
- Brelot A, Chakrabarti LA. CCR4 revisited: how mechanisms of HIV entry govern AIDS pathogenesis. J Mol Biol. 2018;430:2557–2589. - PubMed
-
- Covino DA, Sabbatucci M, Fantuzzi L. The CCL2/CCR2 axis in the pathogenesis of HIV-1 infection: a new cellular target for therapy? Curr Drug Targets. 2016;17:76–110. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
