

Early-onset pancreatic cancer: a population-based study using the SEER registry
- PMID: 31377855
- PMCID: PMC6713682
- DOI: 10.1007/s00423-019-01810-0
Early-onset pancreatic cancer: a population-based study using the SEER registry
Abstract
Background: Early-onset pancreatic cancer (< 50 years, EOPC) is uncommon and limited data exist on clinical presentation and long-term survival. The aim of this study was to compare outcomes between patients with EOPC and those with later-onset pancreatic cancer (≥ 50 years, LOPC) using a large population-based cohort.
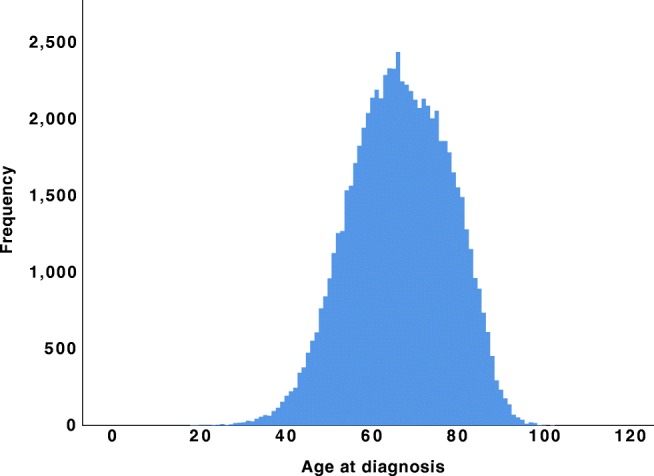
Methods: The Surveillance, Epidemiology, and End Results (SEER) database was queried to identify patients with a microscopically confirmed pancreatic ductal adenocarcinoma for the period 2004 to 2016. Propensity score matching was used to compare overall survival (OS) and cancer-specific survival (CSS) between patients with EOPC and LOPC. The EOPC and LOPC patients were paired 1:1 on propensity scores based on gender, tumor location, tumor size, AJCC stage, and treatment details.
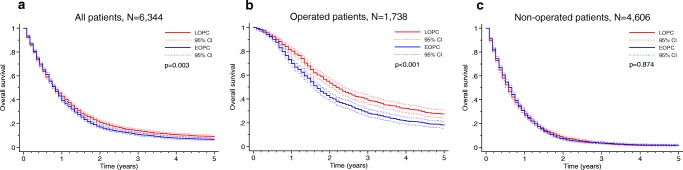
Results: The overall cohort included 72,906 patients with pancreatic ductal adenocarcinoma, including 4523 patients with EOPC (6.2%). EOPC patients were diagnosed at a more advanced AJCC stage (p < 0.001) compared with LOPC patients and received significantly more treatment, including surgery (p < 0.001), radiation (p < 0.001), and chemotherapy (p < 0.001). Following propensity score matching, 3172 EOPC patients were matched to 3172 LOPC patients, alleviating any covariate differences between the groups. The matched analysis showed that EOPC was associated with poorer 5-year OS (6.1% vs 8.6%, p = 0.003) and 5-year CSS (6.7% vs 9.7%, p < 0.001). In multivariable Cox regression analysis, EOPC remained significantly associated with adverse OS and CSS. Subgroup analyses showed that EOPC was associated with adverse 5-year OS (17.7% vs 26.9%, p < 0.001) and 5-year CSS (18.9% vs 29.7%, p < 0.001) in operated patients. After multivariable analysis, EOPC remained significantly associated with OS and CSS. For patients that did not undergo surgery, the OS and CSS remained dismal without any significant differences between the groups.
Conclusion: To our knowledge, this is the largest study to compare the outcome of EOPC vs LOPC, as well as the first to use propensity score matching methodology for this purpose. The findings demonstrate that EOPC is diagnosed at a later stage and the matched survival analysis demonstrated reduced OS and CSS. We suggest that pancreatic cancer in young patients may have a unique tumor biology, which may be of importance for risk stratification and patient counseling.
Keywords: EOPC; Early-onset pancreatic cancer; Population-based study; Propensity score matching; SEER.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
