Comparison of breast tissue markers for tumor localization in breast cancer patients undergoing neoadjuvant chemotherapy
- PMID: 31378014
- PMCID: PMC6769188
- DOI: 10.14366/usg.19004
Comparison of breast tissue markers for tumor localization in breast cancer patients undergoing neoadjuvant chemotherapy
Abstract
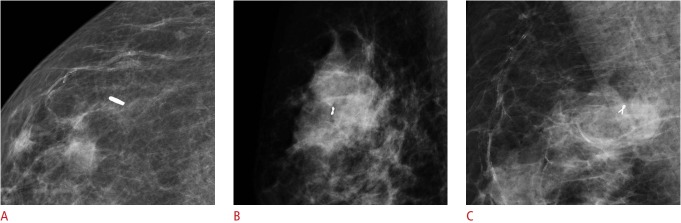
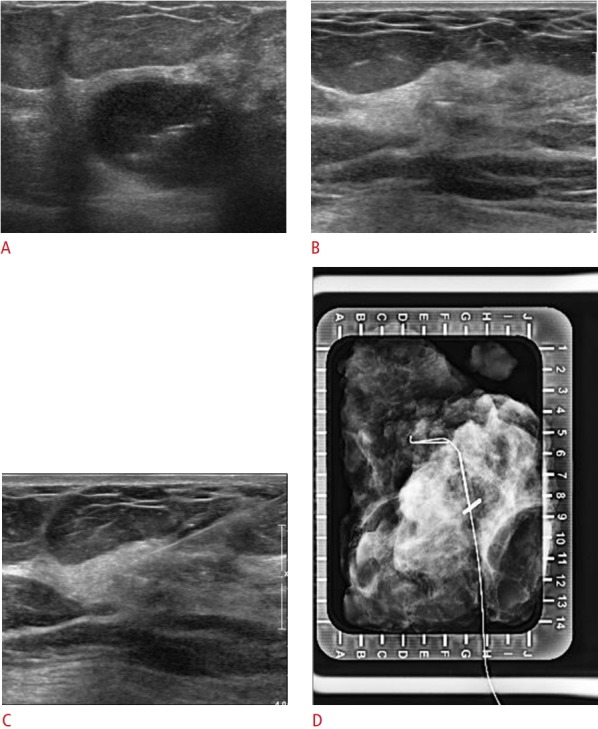
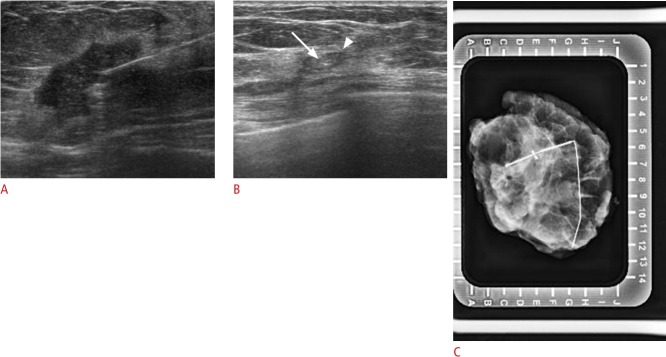
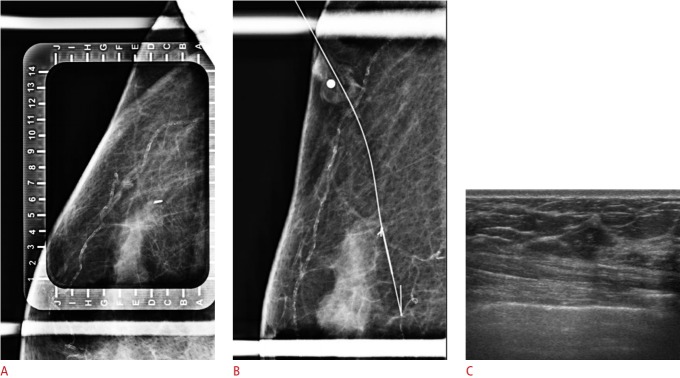
Purpose: The purpose of this study was to compare the visibility of breast tissue markers in cases of breast cancer on ultrasonography (US) after neoadjuvant chemotherapy (NAC) and to analyze whether the type of marker affected the choice of localization method after NAC.
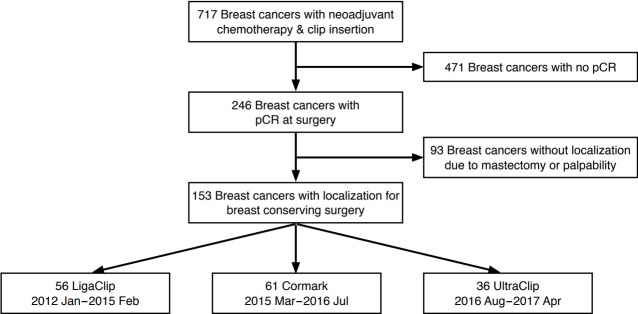
Methods: We included 153 tissue markers inserted within breast cancers that showed pathologically complete response (pCR) after NAC from January 2012 to April 2017. One of three types of markers (a surgical clip, Cormark, or UltraClip) was inserted. Medical records and imaging findings were retrospectively reviewed. We compared the visibility of the different types of tissue markers on US after NAC, and also compared the imaging modalities used in the preoperative localization. The chi-square test, Fisher exact test, and multiple logistic regression were used for analysis.
Results: Of the 153 tissue markers, 56 were surgical clips, 61 Cormark, and 36 UltraClip. After NAC, residual lesions were not seen on US in 42 cases (27.5%). In multivariate analysis, the visibility of the surgical clips and Cormark markers was better than that of the UltraClip markers (odds ratio [OR], 5.467; 95% confidence interal [CI], 1.717 to 17.410; P=0.004 and OR, 3.045; 95% CI, 1.074 to 8.628; P=0.036, respectively). Among the 131 cases where localization targeting the marker was required, the proportion of US-guided localizations was significantly higher when a surgical clip was used than when an UltraClip marker was used (OR, 5.566; 95% CI, 1.610 to 19.246; P=0.007) in the multivariate analysis.
Conclusion: The type of breast tissue marker affected its visibility on US in cases with pCR after NAC, which in turn affected the localization methodology.
Keywords: Breast; Localization; Surgical clip; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Kaufmann M, von Minckwitz G, Mamounas EP, Cameron D, Carey LA, Cristofanilli M, et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surg Oncol. 2012;19:1508–1516. - PubMed
-
- Kaufmann M, Hortobagyi GN, Goldhirsch A, Scholl S, Makris A, Valagussa P, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: an update. J Clin Oncol. 2006;24:1940–1949. - PubMed
-
- Edeiken BS, Fornage BD, Bedi DG, Singletary SE, Ibrahim NK, Strom EA, et al. US-guided implantation of metallic markers for permanent localization of the tumor bed in patients with breast cancer who undergo preoperative chemotherapy. Radiology. 1999;213:895–900. - PubMed
-
- Phillips SW, Gabriel H, Comstock CE, Venta LA. Sonographically guided metallic clip placement after core needle biopsy of the breast. AJR Am J Roentgenol. 2000;175:1353–1355. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous