

Confocal-Assisted Multispectral Fluorescent Microscopy for Brain Tumor Surgery
- PMID: 31380264
- PMCID: PMC6657348
- DOI: 10.3389/fonc.2019.00583
Confocal-Assisted Multispectral Fluorescent Microscopy for Brain Tumor Surgery
Abstract
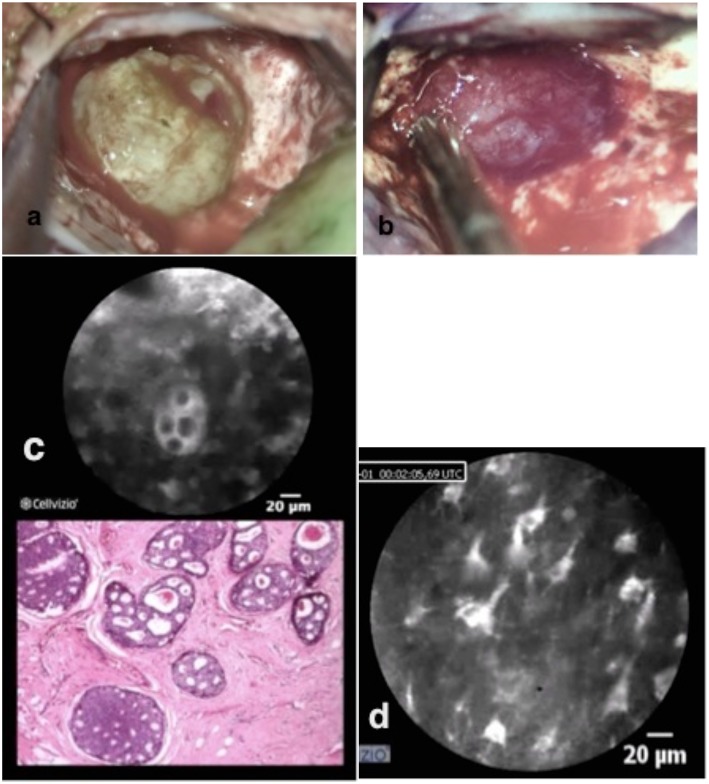
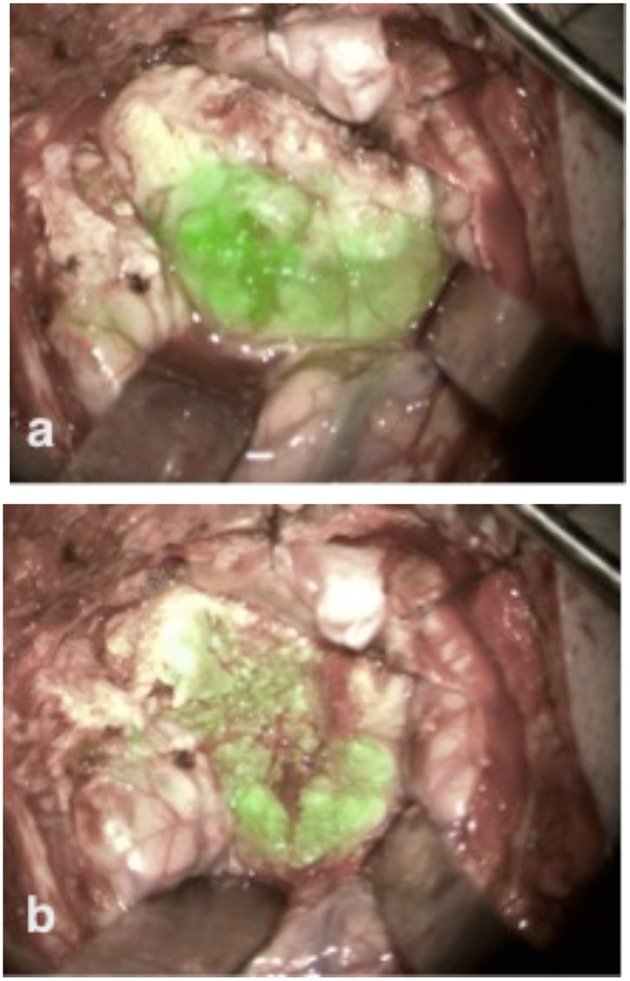
Optimal surgical therapy for brain tumors is the combination of complete resection with minimal invasion and damage to the adjacent normal tissue. To achieve this goal, we need advanced imaging techniques on a scale from macro- to microscopic resolution. In the last decade, the development of fluorescence-guided surgery has been the most influential breakthrough, marginally improving outcomes in brain tumor surgery. Multispectral fluorescence microscopy (MFL) is a novel imaging technique that allows the overlapping of a fluorescent image and a white light image in real-time, with delivery of the merged image to the surgeon through the eyepieces of a surgical microscope. MFL permits the detection and characterization of brain tumors using fluorescent molecular markers such as 5-aminolevulinic acid (5-ALA) or indocyanine green (ICG), while simultaneously obtaining high definition white light images to create a pseudo-colored composite image in real-time. Limitations associated with the use of MFL include decreased light imaging intensity and decreased levels of magnification that may compromise maximal tumor resection on a cellular scale. Confocal laser endomicroscopy (CLE) is another novel advanced imaging technique that is based on miniaturization of the microscope imaging head in order to provide the possibility of in vivo microscopy at the cellular level. Clear visualization of the cellular cytoarchitecture can be achieved with 400-fold-1,000-fold magnification. CLE allows on the one hand the intra-operative detection and differentiation of single tumor cells (without the need for intra-operative histologic analysis of biopsy specimens) as well as the definition of borders between tumor and normal tissue at a cellular level, dramatically improving the accuracy of surgical resection. The application and implementation of CLE-assisted surgery in surgical oncology increases not only the number of options for real-time diagnostic imaging, but also the therapeutic options by extending the resection borders of cancer at a cellular level and, more importantly, by protecting the functionality of normal tissue in the adjacent areas of the human brain. In this article, we describe our experience using these new techniques of confocal-assisted fluorescent surgery including analysis on the technology, usability, indications, limitations, and further developments.
Keywords: brain tumor; confocal laser endomicroscopy (CLE); fluorescent microscopy; meningioma; surgery.
Figures


References
-
- Nickele C, Nguyen V, Fisher W, Couldwell W, Aboud E, David C, et al. A pilot comparison of multispectral fluorescence to indocyanine green videoangiography and other modalities for intraoperative assessment in vascular neurosurgery. Oper Neurosurg (Hagerstown). (2018) 17:103–9. 10.1093/ons/opy237 - DOI - PubMed
LinkOut - more resources
Full Text Sources