

Interoptic, Trans-lamina Terminalis, Opticocarotid Triangle, and Caroticosylvian Windows From Mini-Supraorbital, Frontomedial, and Pterional Perspectives: A Comparative Cadaver Study With Artificial Lesions
- PMID: 31380387
- PMCID: PMC6646665
- DOI: 10.3389/fsurg.2019.00040
Interoptic, Trans-lamina Terminalis, Opticocarotid Triangle, and Caroticosylvian Windows From Mini-Supraorbital, Frontomedial, and Pterional Perspectives: A Comparative Cadaver Study With Artificial Lesions
Abstract
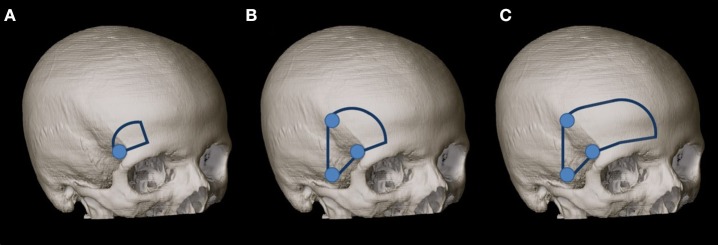
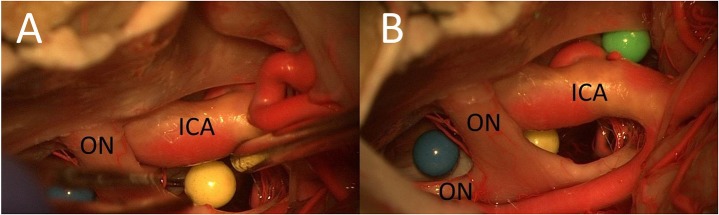
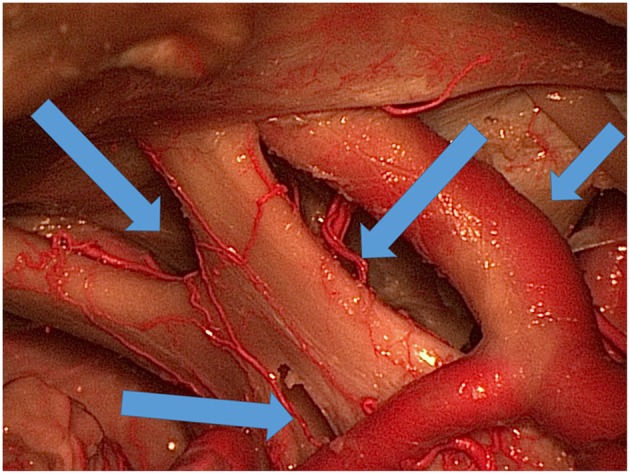
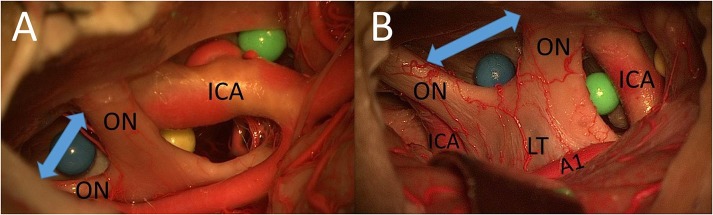
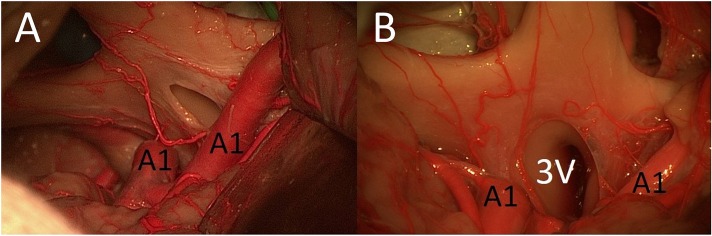
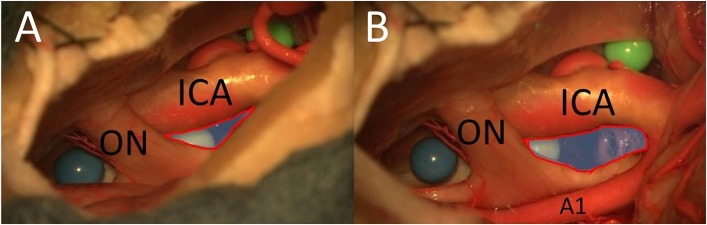
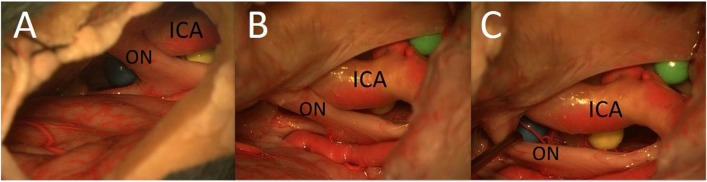
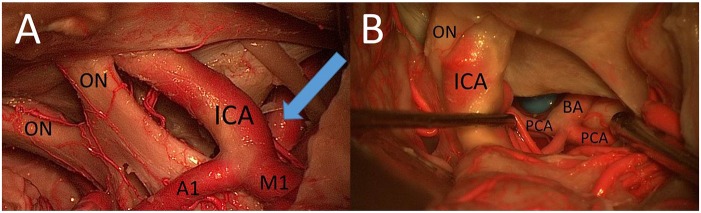
Introduction: The mini-supraorbital (MSO) and pterional (PT) approaches have been compared in a number of studies focusing on the treatment of aneurysms, craniopharyngiomas, and meningiomas. The goal of this study was to analyze the surgical exposure to different artificial lesions through interoptic (IO), trans-lamina terminalis (TLT), opticocarotid triangle (OCT), and caroticosylvian (CS) windows from the MSO, frontomedial (FM), and PT perspectives. Methods: The MSO, PT, and FM approaches were performed sequentially in two fixed cadaver heads. Three colored spheres were placed around the optic chiasm: (1) between the optic nerves; (2) between the optic nerve and the internal carotid artery; and (3) between the internal carotid artery and the oculomotor nerve. The surgical exposures to these structures by using the IO, TLT, OCT, and CS windows were compared. Results: (1) IO window: from the MSO and PT approaches, the total surgical exposure mainly allows visualization of contralateral lesions. The FM approach was superior for exploration of both sides of the area between the optic nerves. (2) TLT pathway: the MSO and PT approaches mainly expose the contralateral third ventricle wall. (3) OCT window: the PT approach allows exposure of a larger part of the sphere between the optic nerve and the internal carotid artery than the MSO approach. (4) CS window: the PT approach allows a better exposure of lateral structures such as the oculomotor nerve and of the medial prepontine area in comparison to the MSO approach. Conclusion: Simulation of the surgical situation with artificial lesions is a good model for comparing surgical perspectives and for analyzing feasibility of lesion exposure and resection.
Keywords: artificial lesions; caroticosylvian window; interoptic window; opticocarotid triangle window; trans-lamina terminalis approach.
Figures
References
-
- Yasargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol. (1975) 3:7–14. - PubMed
LinkOut - more resources
Full Text Sources