

The benefit zone of full-endoscopic spine surgery
- PMID: 31380492
- PMCID: PMC6626753
- DOI: 10.21037/jss.2019.04.19
The benefit zone of full-endoscopic spine surgery
Abstract
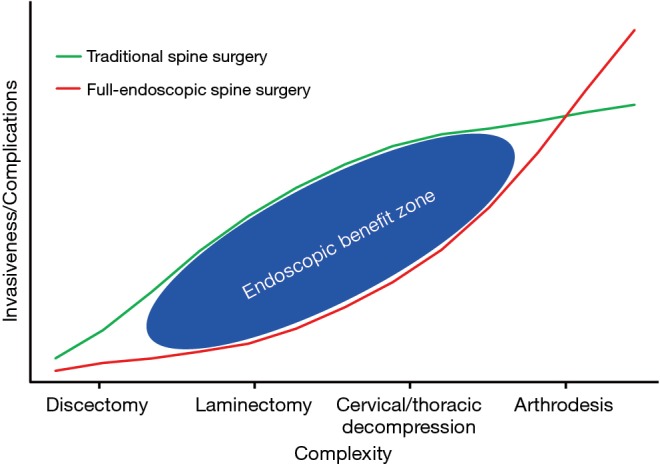
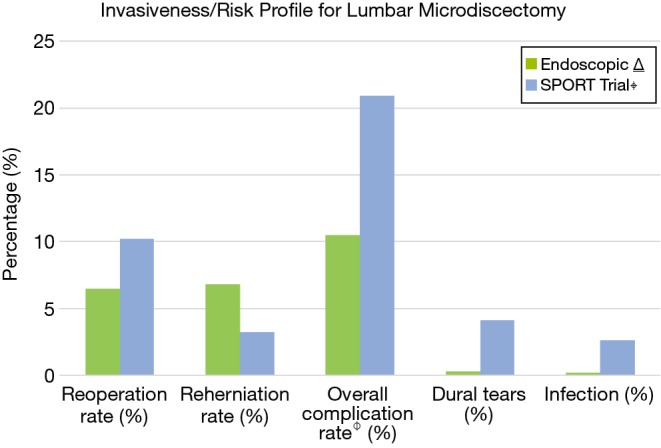
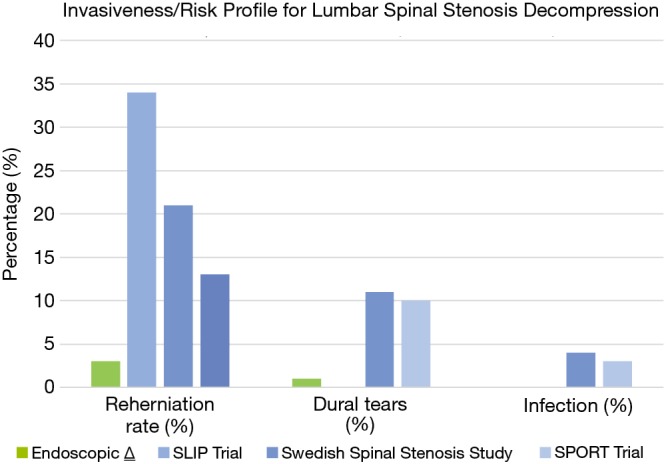
Minimally invasive spine procedures have undergone rapid development during the last decade. Efforts to decrease muscle crush injuries during prolonged retraction, avoid significant soft tissue stripping and minimize bony resection are surgical principles that are employed to prevent iatrogenic instability and provide patients with decreased post-operative pain and disability. Full-endoscopic spine surgery represents a tool for the spine surgeon to provide targeted access to spinal pathology utilizing these principles. Endoscopic techniques have seen over 30 years of evolution and innovation, however, early iterations of these techniques largely focused on transforaminal lumbar microdiscectomies. Currently, endoscopic techniques are utilized for approaching pathology in the cervical, thoracic and lumbar spine. There has been a growing body of literature that not only confirms the efficacy of these procedures but also underscores the advantages these procedures offer with respect to less morbidity and safer complication profiles. Endoscopic decompressions have been utilized in the settings of degenerative spinal stenosis, spondylolisthesis, scoliosis, previous fusion, tumor and infection. Furthermore, endoscopic interbody fusion has also been utilized in the lumbar spine as technology continues to advance. As technological innovation continues to facilitate reproducible surgical technique and expand the indications for use, we believe that endoscopic spine surgical techniques will provide surgeons with a more powerful and less morbid approach to spinal pathology that ultimately elevates the standard of care when treating our patients. We present a brief review of the history of endoscopic spine surgery, an overview of current techniques and review current outcomes of endoscopic spine surgical procedures in the context of an invasiveness/complexity index to elucidate the benefit zone of these newer techniques.
Keywords: Endoscopic spine surgery; invasiveness index; minimally invasive spine surgery.
Conflict of interest statement
Conflicts of Interest: CP Hofstetter: consulting and teaching for J&J, Globus and Joimax; R Hârtl: consultant brainlab DPS. S Hasan has no conflicts of interest to declare.
Figures
References
-
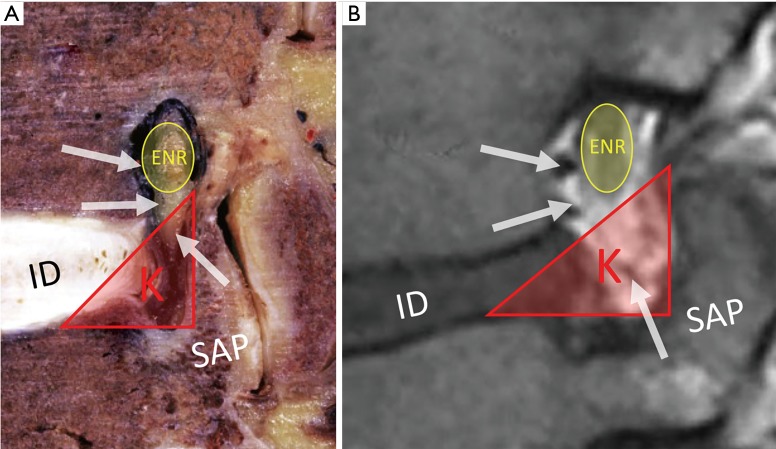
- Kambin P, Brager MD. Percutaneous posterolateral discectomy. Anatomy and mechanism. Clin Orthop Relat Res 1987;(223):145-54. - PubMed
-
- Komp M, Hahn P, Oezdemir S, et al. Bilateral spinal decompression of lumbar central stenosis with the full-endoscopic interlaminar versus microsurgical laminotomy technique: a prospective, randomized, controlled study. Pain Physician 2015;18:61-70. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials