

Ultrasound-guided access to the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: a technical guide
- PMID: 31380781
- PMCID: PMC9724968
- DOI: 10.4244/EIJ-D-19-00555
Ultrasound-guided access to the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: a technical guide
Abstract
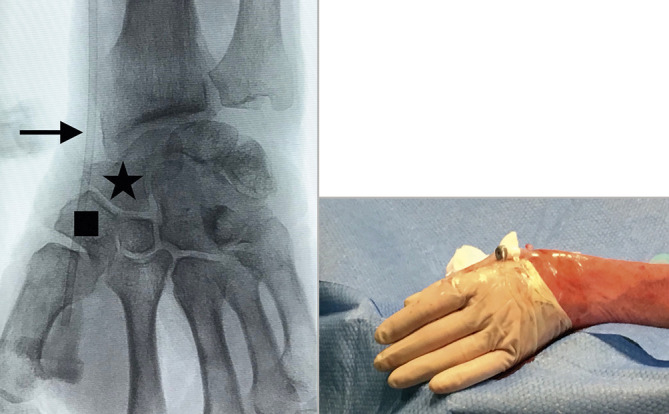
Conventional radial access has been shown to have many advantages over the transfemoral approach. The risk of potential radial artery occlusion and subsequent hand ischaemia can be reduced further by accessing the vessel distally at the anatomical snuffbox, allowing maintenance of antegrade flow to the hand by the superficial palmar arch branch. Additional potential advantages of distal radial access in comparison to the conventional radial approach at the wrist include fewer puncture-site complications and faster post-procedural haemostasis as the vessel is very superficial. Furthermore, it provides another safe, non-femoral option for vascular access. The use of ultrasound guidance enables the operator to identify important anatomical landmarks and avoid injuring adjacent structures. We provide a detailed step-by-step guide for performing distal radial access using sonographic and anatomical correlation, thereby facilitating safe access and optimising technical success.
Conflict of interest statement
S. Nathan is a consultant for Medtronic, Merit Medical and Terumo Interventional Systems. F. Kiemeneij is a consultant for Merit Medical. D. Klass is a consultant for Merit Medical. The other author has no conflicts of interest to declare.
Figures

References
-
- Chase AJ, Fretz EB, Warburton WP, Klinke WP, Carere RG, Pi D, Berry B, Hilton JD. Association of the arterial access site at angioplasty with transfusion and mortality: the M.O.R.T.A.L study (Mortality benefit Of Reduced Transfusion after percutaneous coronary intervention via the Arm or Leg). Heart. 2008;94:1019–25. doi: 10.1136/hrt.2007.136390. - DOI - PubMed
-
- Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimský P, Budaj A, Niemelä M, Valentin V, Lewis BS, Avezum A, Steg PG, Rao SV, Gao P, Afzal R, Joyner CD, Chrolavicius S, Mehta SR RIVAL trial group. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377:1409–20. - PubMed
-
- Valgimigli M, Gagnor A, Calabro P, Frigoli E, Leonardi S, Zaro T, Rubartelli P, Briguori C, Ando G, Repetto A, Limbruno U, Cortese B, Sganzerla P, Lupi A, Galli M, Colangelo S, Ierna S, Ausiello A, Presbitero P, Sardella G, Varbella F, Esposito G, Santarelli A, Tresoldi S, Nazzaro M, Zingarelli A, de Cesare N, Rigattieri S, Tosi P, Palmieri C, Brugaletta S, Rao SV, Heg D, Rothenbuhler M, Vranckx P, Jüni P MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385:2465–76. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical