

Perioperative Management of Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant
- PMID: 31380891
- PMCID: PMC6686768
- DOI: 10.1001/jamainternmed.2019.2431
Perioperative Management of Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant
Abstract
Importance: Patients with atrial fibrillation (AF) who use a direct oral anticoagulant (DOAC) and request elective surgery or procedure present a common clinical situation yet perioperative management is uncertain.
Objective: To investigate the safety of a standardized perioperative DOAC management strategy.
Design, setting, and participants: The Perioperative Anticoagulation Use for Surgery Evaluation (PAUSE) cohort study conducted at 23 clinical centers in Canada, the United States, and Europe enrolled and screened patients from August 1, 2014, through July 31, 2018. Participants (n = 3007) had AF; were 18 years of age or older; were long-term users of apixaban, dabigatran etexilate, or rivaroxaban; were scheduled for an elective surgery or procedure; and could adhere to the DOAC therapy interruption protocol.
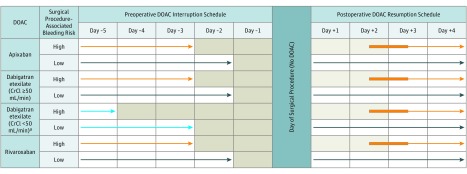
Interventions: A simple standardized perioperative DOAC therapy interruption and resumption strategy based on DOAC pharmacokinetic properties, procedure-associated bleeding risk, and creatinine clearance levels. The DOAC regimens were omitted for 1 day before a low-bleeding-risk procedure and 2 days before a high-bleeding-risk procedure. The DOAC regimens were resumed 1 day after a low-bleeding-risk procedure and 2 to 3 days after a high-bleeding-risk procedure. Follow-up of patients occurred for 30 days after the operation.
Main outcomes and measures: Major bleeding and arterial thromboembolism (ischemic stroke, systemic embolism, and transient ischemic attack) and the proportion of patients with an undetectable or minimal residual anticoagulant level (<50 ng/mL) at the time of the procedure.
Results: The 3007 patients with AF (mean [SD] age of 72.5 [9.39] years; 1988 men [66.1%]) comprised 1257 (41.8%) in the apixaban cohort, 668 (22.2%) in the dabigatran cohort, and 1082 (36.0%) in the rivaroxaban cohort; 1007 patients (33.5%) had a high-bleeding-risk procedure. The 30-day postoperative rate of major bleeding was 1.35% (95% CI, 0%-2.00%) in the apixaban cohort, 0.90% (95% CI, 0%-1.73%) in the dabigatran cohort, and 1.85% (95% CI, 0%-2.65%) in the rivaroxaban cohort. The rate of arterial thromboembolism was 0.16% (95% CI, 0%-0.48%) in the apixaban cohort, 0.60% (95% CI, 0%-1.33%) in the dabigatran cohort, and 0.37% (95% CI, 0%-0.82%) in the rivaroxaban cohort. In patients with a high-bleeding-risk procedure, the rates of major bleeding were 2.96% (95% CI, 0%-4.68%) in the apixaban cohort and 2.95% (95% CI, 0%-4.76%) in the rivaroxaban cohort.
Conclusions and relevance: In this study, patients with AF who had DOAC therapy interruption for elective surgery or procedure, a perioperative management strategy without heparin bridging or coagulation function testing was associated with low rates of major bleeding and arterial thromboembolism.
Conflict of interest statement
Figures
Comment in
-
[Comment on cardiology publications].Turk Kardiyol Dern Ars. 2019 Dec;47(8):712. Turk Kardiyol Dern Ars. 2019. PMID: 31802778 Turkish. No abstract available.
-
Epidural Catheter Use and Further Issues in Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant.JAMA Intern Med. 2020 Feb 1;180(2):332. doi: 10.1001/jamainternmed.2019.5861. JAMA Intern Med. 2020. PMID: 32011629 No abstract available.
-
Epidural Catheter Use and Further Issues in Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant.JAMA Intern Med. 2020 Feb 1;180(2):332-333. doi: 10.1001/jamainternmed.2019.5864. JAMA Intern Med. 2020. PMID: 32011630 No abstract available.
-
Epidural Catheter Use and Further Issues in Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant-Reply.JAMA Intern Med. 2020 Feb 1;180(2):333-334. doi: 10.1001/jamainternmed.2019.5851. JAMA Intern Med. 2020. PMID: 32011635 No abstract available.
References
-
- Healey JS, Eikelboom J, Douketis J, et al. ; RE-LY Investigators . Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial[published correction appears in Circulation. 2012;126(10):e160]. Circulation. 2012;126(3):343-348. doi:10.1161/CIRCULATIONAHA.111.090464 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
