

Molecular Coronary Plaque Imaging Using 18F-Fluoride
- PMID: 31382765
- PMCID: PMC7668410
- DOI: 10.1161/CIRCIMAGING.118.008574
Molecular Coronary Plaque Imaging Using 18F-Fluoride
Abstract
Background: Coronary 18F-fluoride positron emission tomography identifies ruptured and high-risk atherosclerotic plaque. The optimal method to identify, to quantify, and to categorize increased coronary 18F-fluoride uptake and determine its reproducibility has yet to be established. This study aimed to optimize the identification, quantification, categorization, and scan-rescan reproducibility of increased 18F-fluoride activity in coronary atherosclerotic plaque.
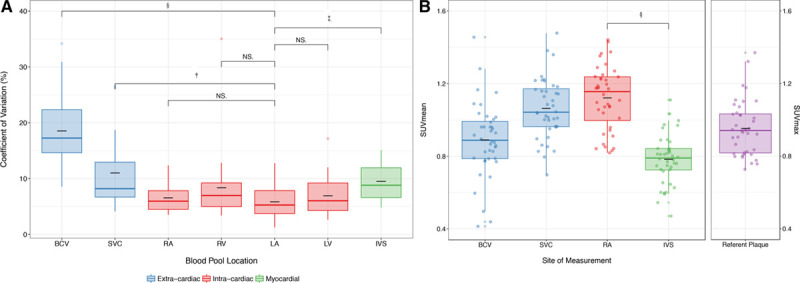
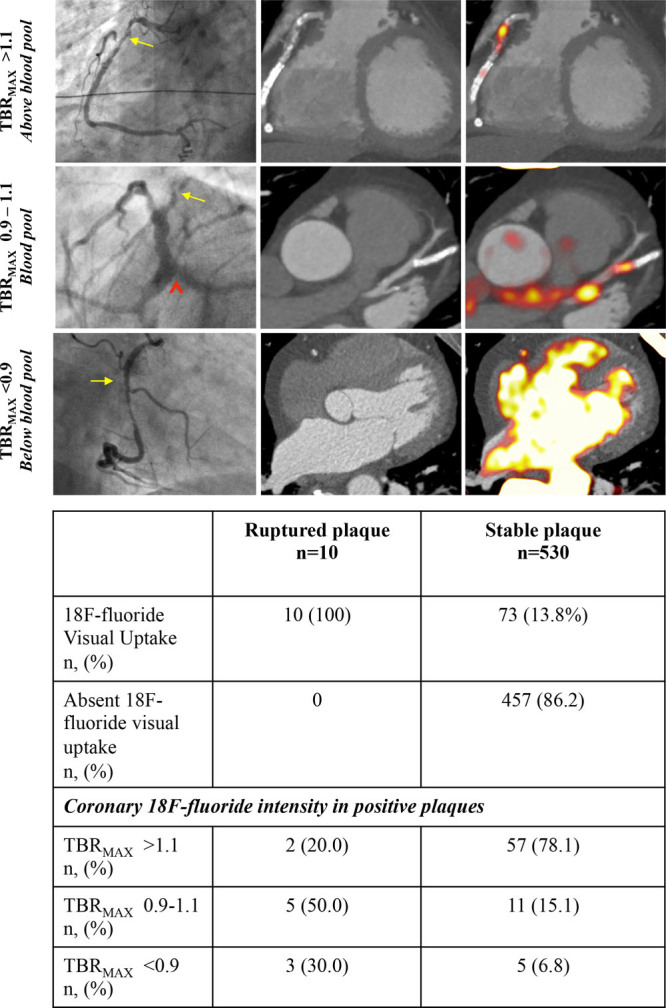
Methods: In a prospective observational study, patients with multi-vessel coronary artery disease underwent serial 18F-fluoride positron emission tomography. Coronary 18F-fluoride activity was visually assessed, quantified, and categorized with reference to maximal tissue to background ratios. Levels of agreement for both visual and quantitative methods were determined between scans and observers.
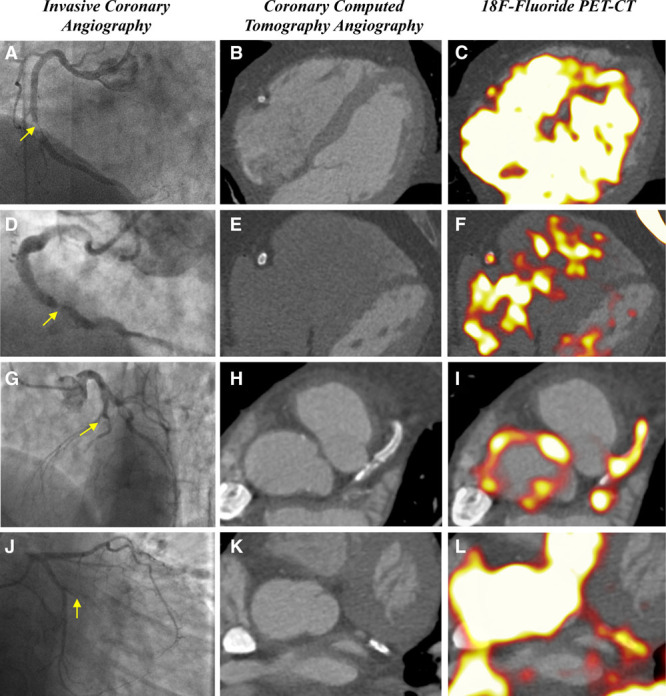
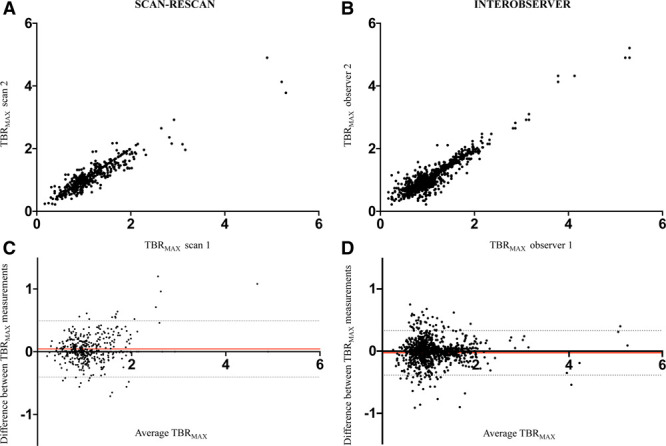
Results: Thirty patients (90% male, 20 patients with stable coronary artery disease, and 10 with recent type 1 myocardial infarction) underwent paired serial positron emission tomography-coronary computed tomography angiography imaging within an interval of 12±5 days. A mean of 3.7±1.8 18F-fluoride positive plaques per patient was identified after recent acute coronary syndrome, compared with 2.4±2.3 positive plaques per patient in stable coronary artery disease. The bias in agreement in maximum tissue to background ratio measurements in visually positive plaques was low between observers (mean difference, -0.01; 95% limits of agreement, -0.32 to 0.30) or between scans (mean difference, 0.06; 95% limits of agreement, -0.49 to 0.61). Good agreement in the categorization of focal 18F-fluoride uptake was achieved using visual assessment alone (κ=0.66) and further improved at higher maximum tissue to background ratio values.
Conclusions: Coronary 18F-fluoride activity is a precise and reproducible metric in the coronary vasculature. The analytical performance of 18F-fluoride is sufficient to assess the prognostic utility of this radiotracer as a noninvasive imaging biomarker of plaque vulnerability.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifiers: NCT02110303 and NCT02278211.
Keywords: angiography; computed tomography angiography; coronary artery disease; fluorides; myocardial infarction.
Figures
Comment in
-
Hype or Hope18F-NaF Positron Emission Tomography for Vulnerable Coronary Plaque Imaging.Circ Cardiovasc Imaging. 2019 Aug;12(8):e009591. doi: 10.1161/CIRCIMAGING.119.009591. Epub 2019 Aug 6. Circ Cardiovasc Imaging. 2019. PMID: 31382767 Free PMC article. No abstract available.
References
-
- Libby P. Mechanisms of acute coronary syndromes and their implications for therapy. N Engl J Med. 2013;368:2004–2013. doi: 10.1056/NEJMra1216063. - PubMed
-
- Van Lierde J, De Geest H, Verstraete M, Van de Werf F. Angiographic assessment of the infarct-related residual coronary stenosis after spontaneous or therapeutic thrombolysis. J Am Coll Cardiol. 1990;16:1545–1549. doi: 10.1016/0735-1097(90)90298-4. - PubMed
-
- Chang HJ, Lin FY, Lee SE, Andreini D, Bax J, Cademartiri F, Chinnaiyan K, Chow BJW, Conte E, Cury RC, Feuchtner G, Hadamitzky M, Kim YJ, Leipsic J, Maffei E, Marques H, Plank F, Pontone G, Raff GL, van Rosendael AR, Villines TC, Weirich HG, Al’Aref SJ, Baskaran L, Cho I, Danad I, Han D, Heo R, Lee JH, Rivzi A, Stuijfzand WJ, Gransar H, Lu Y, Sung JM, Park HB, Berman DS, Budoff MJ, Samady H, Shaw LJ, Stone PH, Virmani R, Narula J, Min JK. Coronary atherosclerotic precursors of acute coronary syndromes. J Am Coll Cardiol. 2018;71:2511–2522. doi: 10.1016/j.jacc.2018.02.079. - PMC - PubMed
-
- Ahmadi A, Leipsic J, Blankstein R, Taylor C, Hecht H, Stone GW, Narula J. Do plaques rapidly progress prior to myocardial infarction? The interplay between plaque vulnerability and progression. Circ Res. 2015;117:99–104. doi: 10.1161/CIRCRESAHA.117.305637. - PubMed
-
- Dweck MR, Chow MW, Joshi NV, Williams MC, Jones C, Fletcher AM, Richardson H, White A, McKillop G, van Beek EJ, Boon NA, Rudd JH, Newby DE. Coronary arterial 18F-sodium fluoride uptake: a novel marker of plaque biology. J Am Coll Cardiol. 2012;59:1539–1548. doi: 10.1016/j.jacc.2011.12.037. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- G0701127/MRC_/Medical Research Council/United Kingdom
- FS/17/79/33226/BHF_/British Heart Foundation/United Kingdom
- FS/19/17/34172/BHF_/British Heart Foundation/United Kingdom
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- PCL/17/04/CSO_/Chief Scientist Office/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- FS/17/51/33096/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/BHF_/British Heart Foundation/United Kingdom
- RE/13/3/30183/BHF_/British Heart Foundation/United Kingdom
- MC_PC_12040/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
