

Long-term clinical outcomes in patients with untreated non-culprit intermediate coronary lesion and evaluation of predictors by using virtual histology-intravascular ultrasound; a prospective cohort study
- PMID: 31382885
- PMCID: PMC6683474
- DOI: 10.1186/s12872-019-1173-5
Long-term clinical outcomes in patients with untreated non-culprit intermediate coronary lesion and evaluation of predictors by using virtual histology-intravascular ultrasound; a prospective cohort study
Abstract
Background: It is uncertain whether the coronary lesion with intermediate stenosis is more likely to cause cardiovascular events than a normal or minimal lesion. We conducted a single-center, prospective cohort study to identify long-term clinical outcomes of patients with untreated non-culprit intermediate lesion and evaluate its predictor of cardiovascular events by using virtual histology-intravascular ultrasound (VH-IVUS).
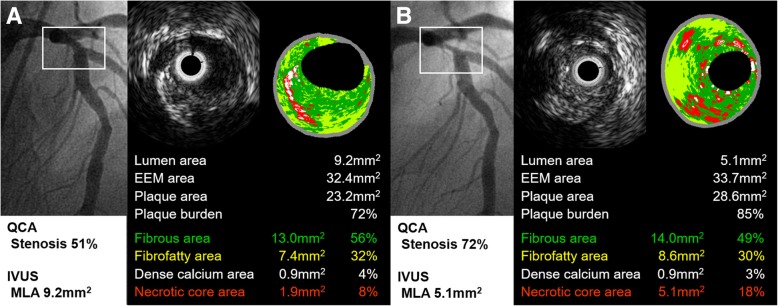
Methods: Subjects with non-culprit intermediate lesion underwent VH-IVUS were prospectively registered after percutaneous coronary intervention at the culprit lesion. Intermediate lesion was defined as 30 to 70% stenosis in coronary angiography and primary outcome was an occurrence of major adverse cardiovascular events (MACE) defined as all-cause death, intermediate lesion revascularization (InLR), minimal lesion revascularization (MnLR, unplanned revascularization elsewhere in the target vessel or in other coronary arteries which looked normal or minimal stenosis), cerebrovascular events, or non-fatal myocardial infarction (MI). The mean follow-up period was 4.2 years.
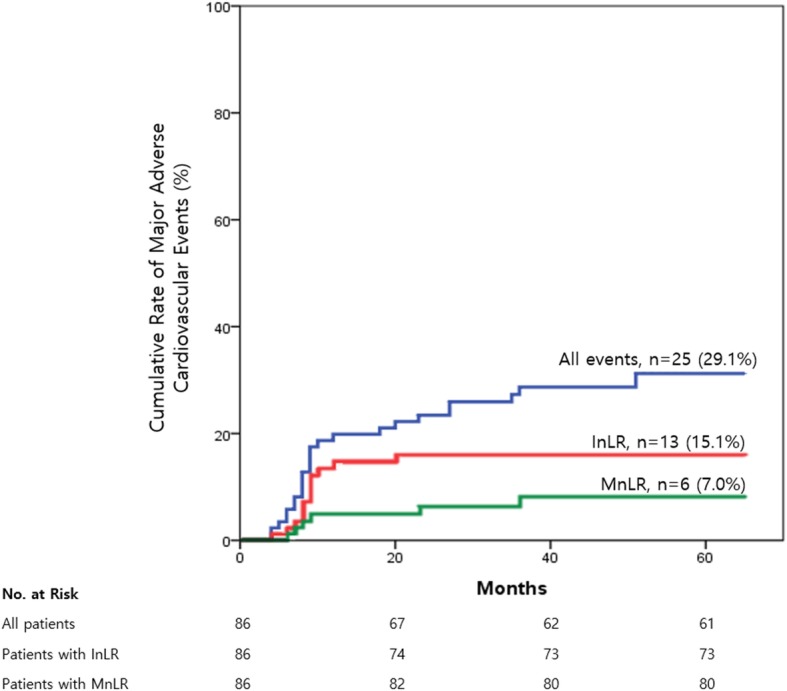
Results: Total 25 MACE, approximately 7% incidence annually, were identified during a follow-up period in 86 patients with 89 intermediate lesions. InLR (n = 13) was a most common event followed by MnLR (n = 6), non-fatal MI (n = 4), all-cause death (n = 3), and cerebrovascular events (n = 1). Diameter stenosis (OR 1.07, 95% CI 1.01-1.12, p = 0.015), plaque burden (PB, OR 1.07, 95% CI 1.00-1.15, p = 0.040), fibrofatty area (FFA, OR 1.61, 95% CI 1.10-2.38, p = 0.016), PB ≥ 70% (OR 3.93, 95% CI 1.28-12.07, p = 0.018), and area stenosis ≥ 50% (OR 2.94, 95% CI 1.01-8.56, p = 0.042) showed significant relationships with an occurrence of MACE. In multivariable Cox-proportional hazard analysis, FFA in intermediate lesion was an only independent predictor of MACE (HR 1.36, 95% CI 1.05-1.77, p = 0.019).
Conclusions: Untreated intermediate lesions had a significantly higher chance for requiring revascularization compared with a normal or minimal lesion. And also, a large FFA in intermediate lesion was a significant predictor of cardiovascular events and which finding was mainly driven by coronary-related events, in particularly intermediate lesion progression.
Keywords: Atherosclerosis; Coronary angiography; Coronary artery disease; Myocardial ischemia; Ultrasonography, interventional.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nam CW, Yoon HJ, Cho YK, Park HS, Kim H, Hur SH, et al. Outcomes of percutaneous coronary intervention in intermediate coronary artery disease: fractional flow reserve-guided versus intravascular ultrasound-guided. JACC Cardiovasc Interv. 2010;3:812–817. doi: 10.1016/j.jcin.2010.04.016. - DOI - PubMed
-
- Calvert PA, Obaid DR, O’Sullivan M, Shapiro LM, McNab D, Densem CG, et al. Association between IVUS findings and adverse outcomes in patients with coronary artery disease: the VIVA (VH-IVUS in vulnerable atherosclerosis) study. JACC Cardiovasc Imaging. 2011;4:894–901. doi: 10.1016/j.jcmg.2011.05.005. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
