

Needle tract seeding following endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a report of two cases
- PMID: 31382964
- PMCID: PMC6683495
- DOI: 10.1186/s12957-019-1681-x
Needle tract seeding following endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a report of two cases
Abstract
Background: Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is a useful tool in pancreatic cancer diagnosis. However, the procedure itself may cause peritoneal dissemination and needle tract seeding at the puncture site. We herein report two cases of gastric wall metastasis due to needle tract seeding after EUS-FNA.
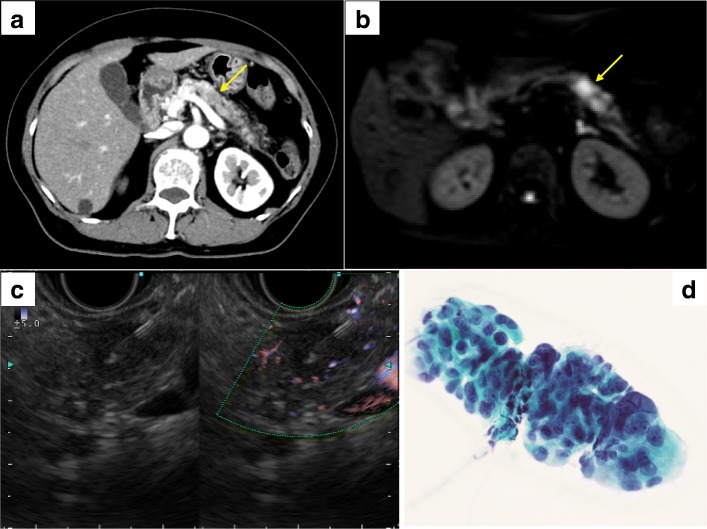
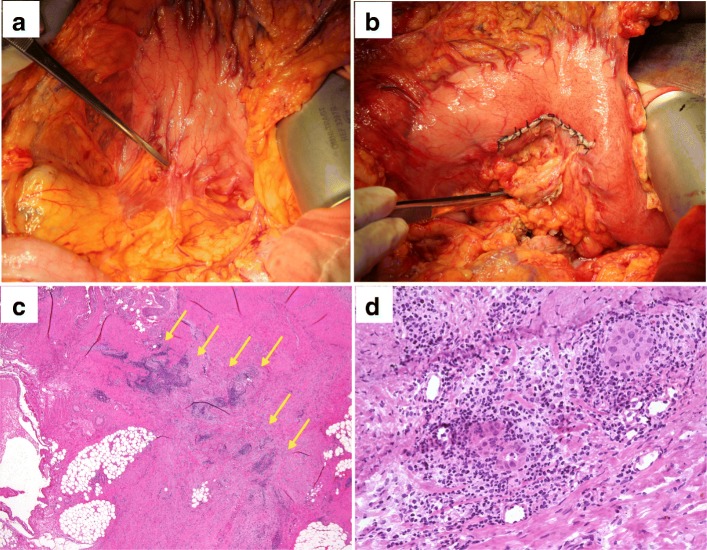
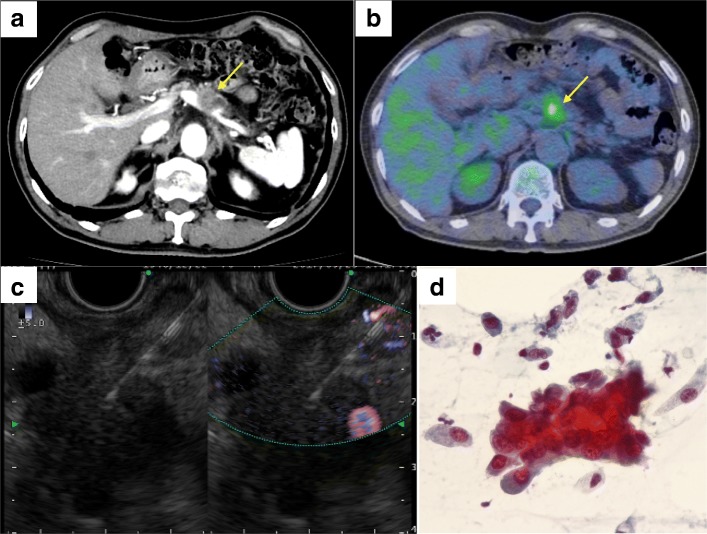
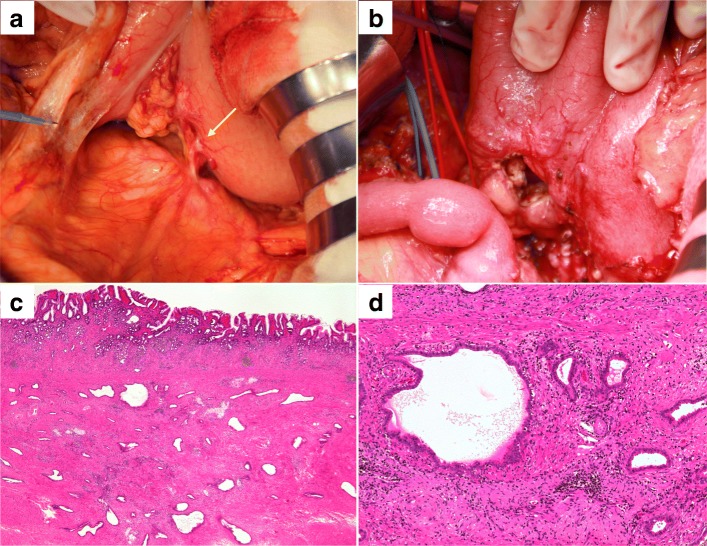
Case presentation: Case 1: A 68-year-old woman was admitted to our hospital for persistent cough. Computed tomography (CT) scan revealed inflammatory changes in the left lung field, and incidentally, a 15-mm hypovascular mass was detected in the pancreatic body. She underwent EUS-FNA and was diagnosed as pancreatic adenocarcinoma. She underwent distal pancreatectomy with splenectomy; however, a small hard mass was observed in the posterior gastric wall during surgery. We performed partial gastrectomy, and the resected specimen was diagnosed as a needle tract seeding following EUS-FNA. She then underwent adjuvant chemotherapy with TS-1, but the pancreatic cancer showed recurrence 6 months after surgery. She died due to peritoneal dissemination 18 months after surgery. Case 2: A 70-year-old man was incidentally detected with a pancreatic body mass on a CT scan as part of his follow-up for recurrence of basal cell carcinoma. He underwent EUS-FNA and was diagnosed as pancreatic adenocarcinoma. He had nodules in both lungs, and it was difficult to differentiate them from lung metastasis of pancreatic cancer. Therefore, he underwent neoadjuvant chemoradiotherapy, and thereafter, the lung nodules showed no changes; hence, he underwent distal pancreatectomy with splenectomy. During surgery, we observed a hard mass in the posterior gastric wall. We performed partial gastrectomy, and the resected specimen was diagnosed as needle tract seeding due to EUS-FNA. He underwent chemotherapy with TS-1, and he is still alive 18 months after surgery at the time of writing.
Conclusion: For resectable pancreatic body or tail tumors, EUS-FNA should be carefully performed to prevent needle tract seeding and intraoperative as well as postoperative assessment for gastric wall metastasis is mandatory.
Keywords: Endoscopic ultrasound-guided fine-needle aspiration; Gastric wall metastasis; Needle tract seeding; Pancreatic cancer; Surgical resection.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Yamauchi J, Kobayashi S, Miyazaki K, Ajiki T, Tsuchihara K, Ishiyama S. A case of curative resection of needle tract seeding after EUS-guided fine needle aspiration for pancreatic body cancer. J Jpn Surg Assoc. 2016;77(12):2994–2999. doi: 10.3919/jjsa.77.2994. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
