

NightBalance Sleep Position Treatment Device Versus Auto-Adjusting Positive Airway Pressure for Treatment of Positional Obstructive Sleep Apnea
- PMID: 31383231
- PMCID: PMC6622520
- DOI: 10.5664/jcsm.7868
NightBalance Sleep Position Treatment Device Versus Auto-Adjusting Positive Airway Pressure for Treatment of Positional Obstructive Sleep Apnea
Abstract
Study objectives: Compare treatment efficacy and objective adherence between the NightBalance sleep position treatment (SPT) device and auto-adjusting positive airway pressure (APAP) in patients with exclusive positional obstructive sleep apnea (ePOSA) defined as a supine apnea-hypopnea index (sAHI) ≥ 2 times the nonsupine AHI (nsAHI) and a nsAHI < 10 events/h.
Methods: This prospective multicenter randomized crossover trial enrolled treatment naive participants with ePOSA (AHI ≥ 15 events/h and nsAHI < 10 events/h) or (AHI > 10 and < 15 events/h with daytime sleepiness and nsAH < 5 events/h). Polysomnography and objective adherence determination (device data) were performed at the end of each 6-week treatment. Patient device preference was determined at the end of the study.
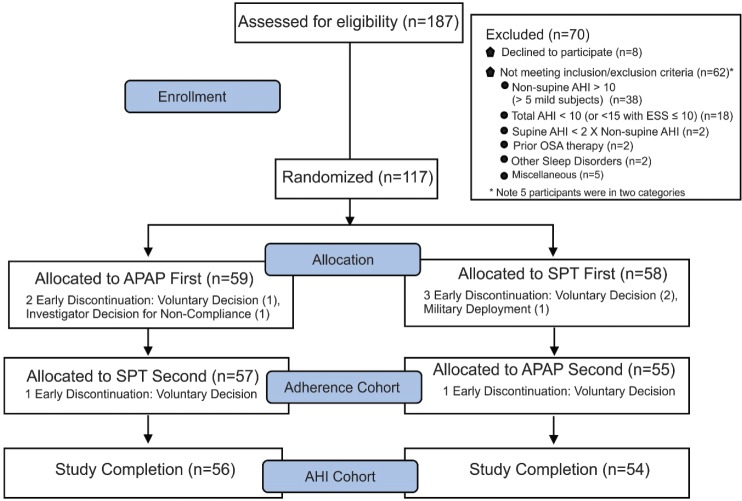
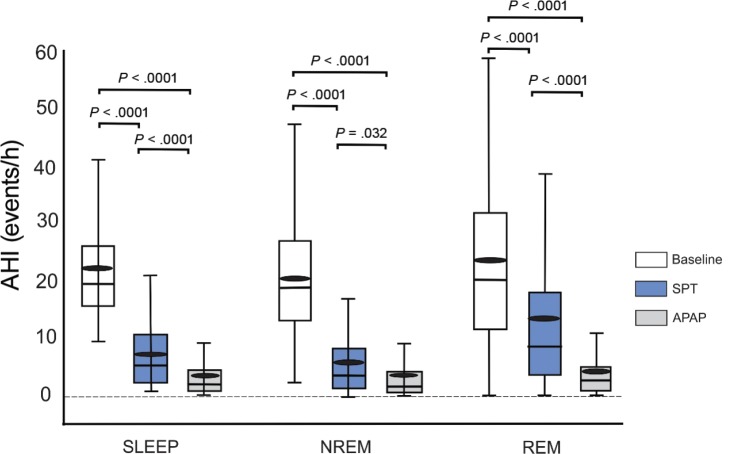
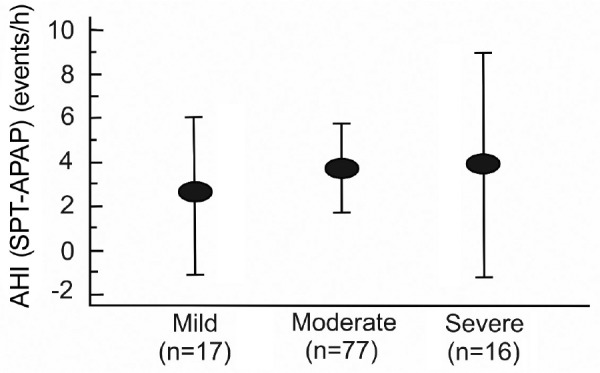
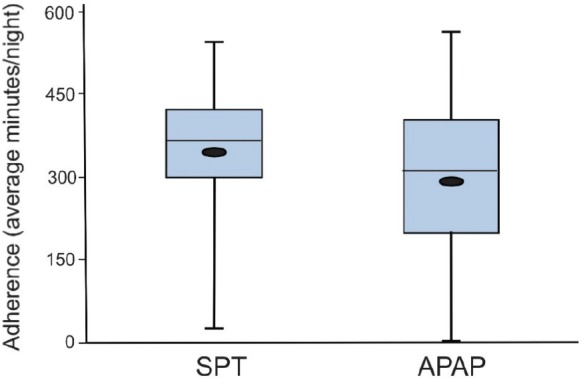
Results: A total of 117 participants were randomized (58 SPT first, 59 APAP first). Of these, 112 started treatment with the second device (adherence cohort) and 110 completed the study (AHI cohort). The AHI on SPT was higher (mean ± standard deviation, 7.29 ± 6.8 versus 3.71 ± 5.1 events/h, P < .001). The mean AHI difference (SPT-APAP) was 3.58 events/h with a one sided 95% confidence interval upper bound of 4.96 events/h (< the prestudy noninferiority margin of 5 events/h). The average nightly adherence (all nights) was greater on SPT (345.3 ± 111.22 versus 286.98 ± 128.9 minutes, P < .0001). Participants found the SPT to be more comfortable and easier to use and 53% reported a preference for SPT assuming both devices were equally effective.
Conclusions: Treatment with SPT resulted in non-inferior treatment efficacy and greater adherence compared to APAP in ePOSA suggesting that SPT is an effective treatment for this group.
Clinical trial registration: Registry: ClinicalTrials.gov; Title: The POSAtive Study: Study for the Treatment of Positional Obstructive Sleep Apnea; Identifier: NCT03061071; URL: https://clinicaltrials.gov/ct2/show/NCT03061071.
Keywords: continuous positive airway pressure; obstructive sleep apnea; position treatment.
Copyright © 2019 American Academy of Sleep Medicine. All rights reserved.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
