

Potentiation of Aminoglycoside Lethality by C4-Dicarboxylates Requires RpoN in Antibiotic-Tolerant Pseudomonas aeruginosa
- PMID: 31383655
- PMCID: PMC6761562
- DOI: 10.1128/AAC.01313-19
Potentiation of Aminoglycoside Lethality by C4-Dicarboxylates Requires RpoN in Antibiotic-Tolerant Pseudomonas aeruginosa
Abstract
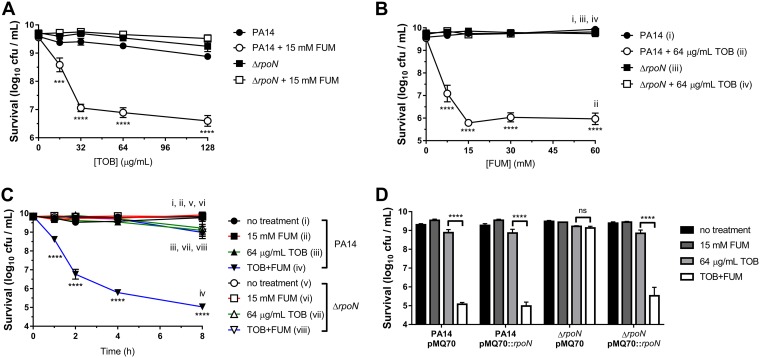
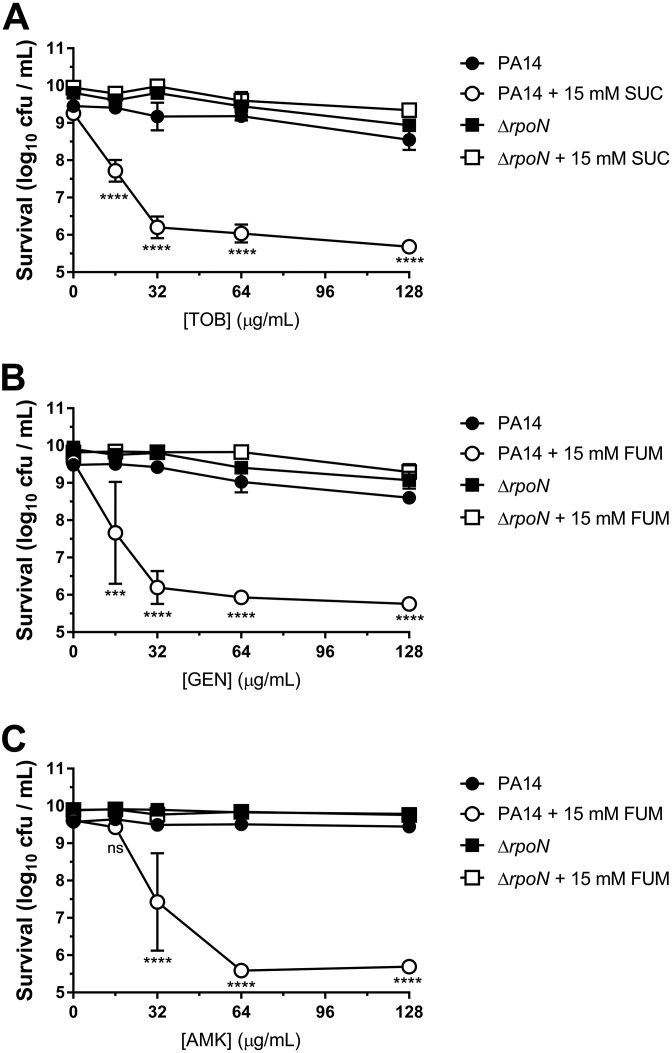
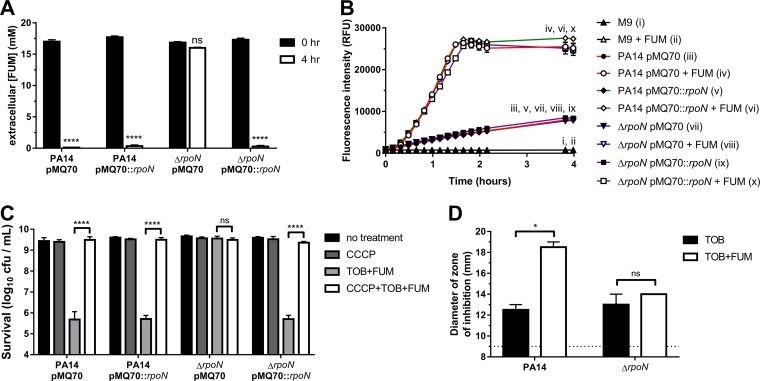
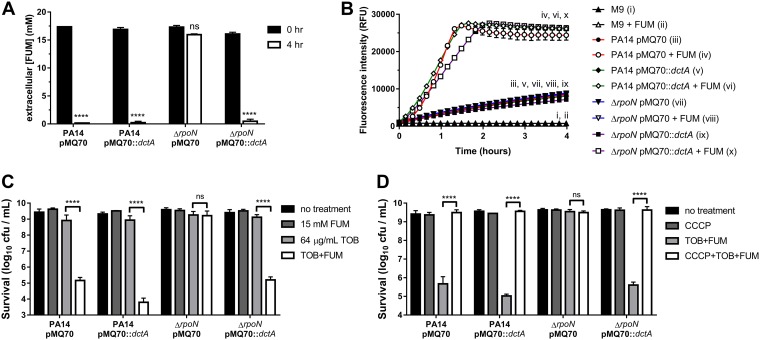
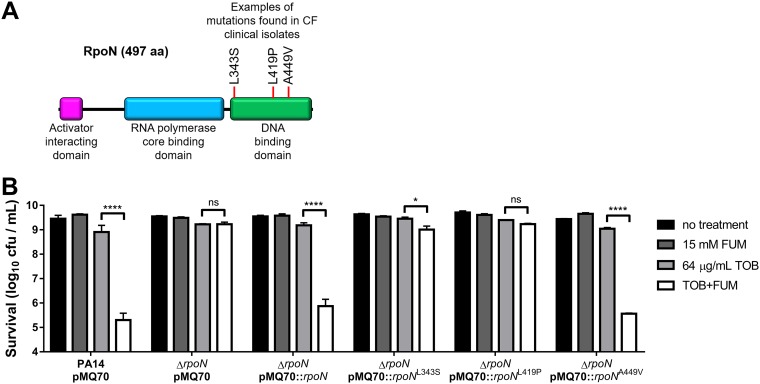
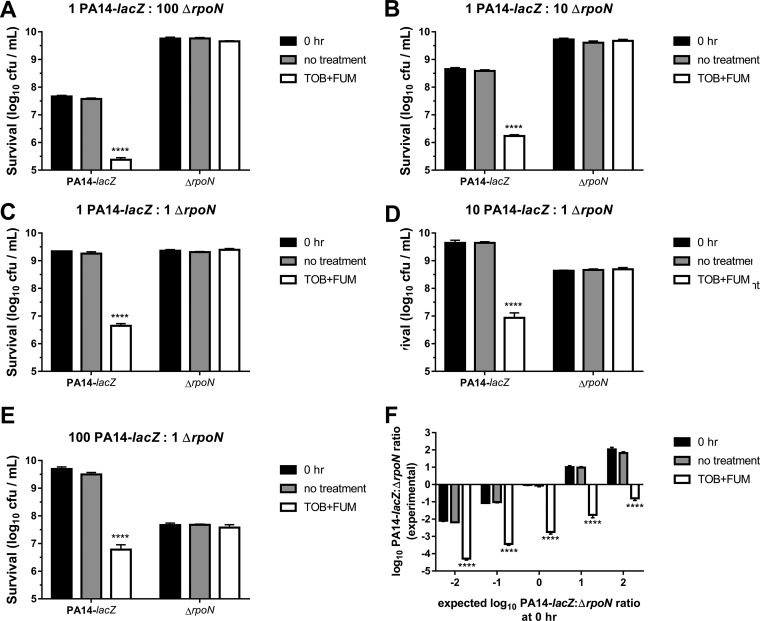
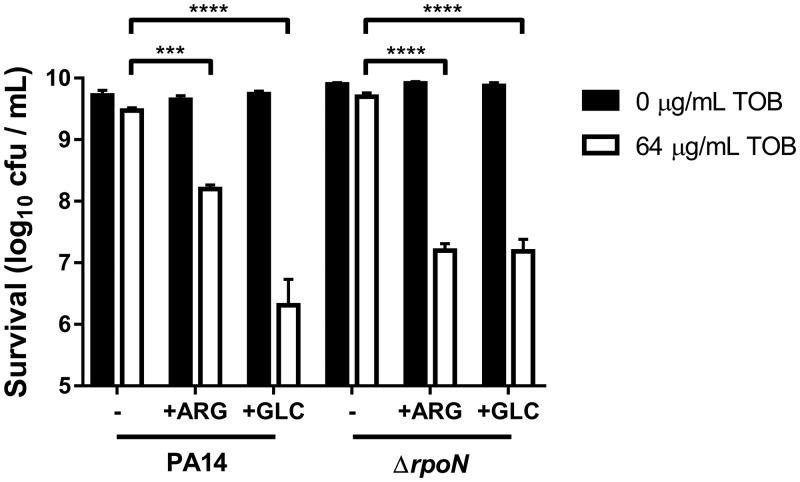
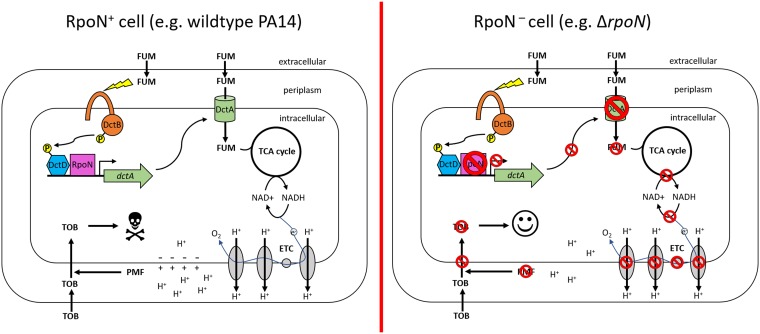
Antibiotic tolerance contributes to the inability of standard antimicrobial therapies to clear the chronic Pseudomonas aeruginosa lung infections that often afflict patients with cystic fibrosis (CF). Metabolic potentiation of bactericidal antibiotics with carbon sources has emerged as a promising strategy to resensitize tolerant bacteria to antibiotic killing. Fumarate (FUM), a C4-dicarboxylate, has been recently shown to resensitize tolerant P. aeruginosa to killing by tobramycin (TOB), an aminoglycoside antibiotic, when used in combination (TOB+FUM). Fumarate and other C4-dicarboxylates are taken up intracellularly by transporters regulated by the alternative sigma factor RpoN. Once in the cell, FUM is metabolized, leading to enhanced electron transport chain activity, regeneration of the proton motive force, and increased TOB uptake. In this work, we demonstrate that a ΔrpoN mutant displays impaired FUM uptake and, consequently, nonsusceptibility to TOB+FUM treatment. RpoN was also found to be essential for susceptibility to other aminoglycoside and C4-dicarboxylate combinations. Importantly, RpoN loss-of-function mutations have been documented to evolve in the CF lung, and these loss-of-function alleles can also result in TOB+FUM nonsusceptibility. In a mixed-genotype population of wild-type and ΔrpoN cells, TOB+FUM specifically killed cells with RpoN function and spared the cells that lacked RpoN function. Unlike C4-dicarboylates, both d-glucose and l-arginine were able to potentiate TOB killing of ΔrpoN stationary-phase cells. Our findings raise the question of whether TOB+FUM will be a suitable treatment option in the future for CF patients infected with P. aeruginosa isolates that lack RpoN function.
Keywords: Pseudomonas aeruginosa; antibiotic tolerance; fumarate; metabolic potentiation; rpoN; tobramycin.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Ramsey BW, Pepe MS, Quan JM, Otto KL, Montgomery AB, Williams-Warren J, Vasiljev-K M, Borowitz D, Bowman CM, Marshall BC, Marshall S, Smith AL. 1999. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med 340:23–30. doi: 10.1056/NEJM199901073400104. - DOI - PubMed
-
- Smith WD, Bardin E, Cameron L, Edmondson CL, Farrant KV, Martin I, Murphy RA, Soren O, Turnbull AR, Wierre-Gore N, Alton EW, Bundy JG, Bush A, Connett GJ, Faust SN, Filloux A, Freemont PS, Jones AL, Takats Z, Webb JS, Williams HD, Davies JC. 2017. Current and future therapies for Pseudomonas aeruginosa infection in patients with cystic fibrosis. FEMS Microbiol Lett 364:fnx121. doi: 10.1093/femsle/fnx121. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
