

Complementary therapies for clinical depression: an overview of systematic reviews
- PMID: 31383703
- PMCID: PMC6686993
- DOI: 10.1136/bmjopen-2018-028527
Complementary therapies for clinical depression: an overview of systematic reviews
Abstract
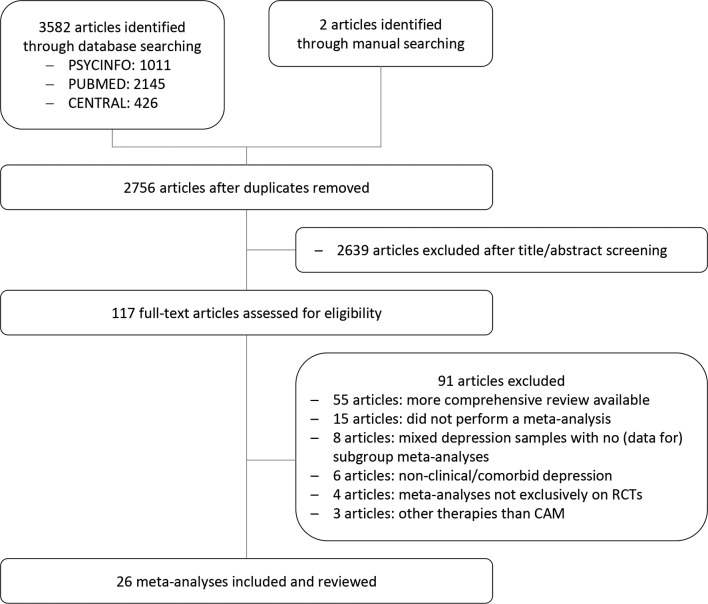
Objectives: As clinical practice guidelines vary widely in their search strategies and recommendations of complementary and alternative medicine (CAM) for depression, this overview aimed at systematically summarising the level 1 evidence on CAM for patients with a clinical diagnosis of depression.
Methods: PubMed, PsycInfo and Central were searched for meta-analyses of randomised controlled clinical trials (RCTs) until 30 June 2018. Outcomes included depression severity, response, remission, relapse and adverse events. The quality of evidence was assessed according to Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) considering the methodological quality of the RCTs and meta-analyses, inconsistency, indirectness, imprecision of the evidence and the potential risk of publication bias.
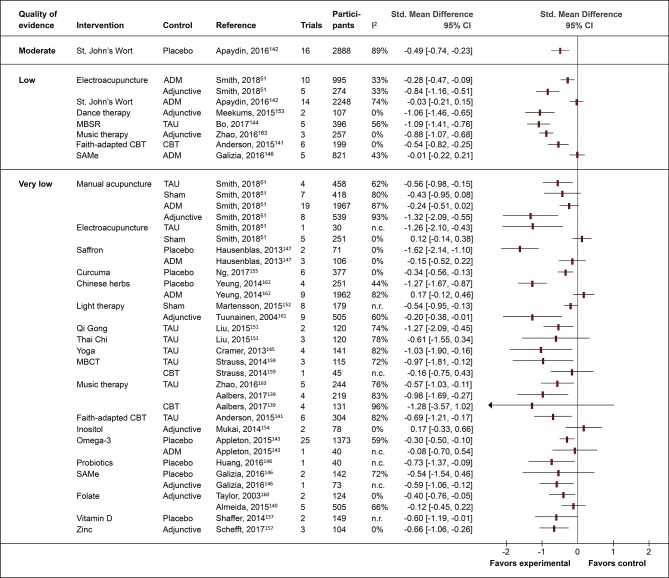
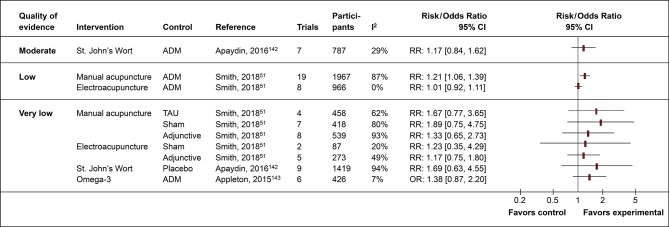
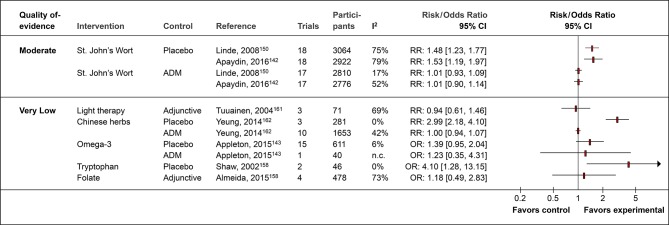
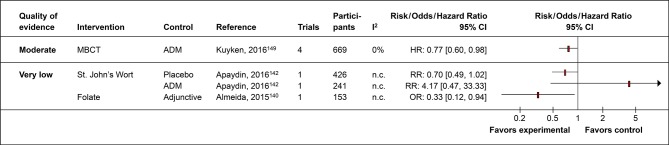
Results: The literature search revealed 26 meta-analyses conducted between 2002 and 2018 on 1-49 RCTs in major, minor and seasonal depression. In patients with mild to moderate major depression, moderate quality evidence suggested the efficacy of St. John's wort towards placebo and its comparative effectiveness towards standard antidepressants for the treatment for depression severity and response rates, while St. John's wort caused significant less adverse events. In patients with recurrent major depression, moderate quality evidence showed that mindfulness-based cognitive therapy was superior to standard antidepressant drug treatment for the prevention of depression relapse. Other CAM evidence was considered as having low or very low quality.
Conclusions: The effects of all but two CAM treatments found in studies on clinical depressed patients based on low to very low quality of evidence. The evidence has to be downgraded mostly due to avoidable methodological flaws of both the original RCTs and meta-analyses not following the Consolidated Standards of Reporting Trials and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Further research is needed.
Keywords: complementary therapies; depression; safety; systematic review; treatment outcome.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- American Psychiatric Association Diagnostic and statistical manual of mental disorders. 5th ed (DSM-5) Arlington: American Psychiatric Publishing, 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials