

Recent advances in research on isolated congenital central hypothyroidism
- PMID: 31384098
- PMCID: PMC6646241
- DOI: 10.1297/cpe.28.69
Recent advances in research on isolated congenital central hypothyroidism
Abstract
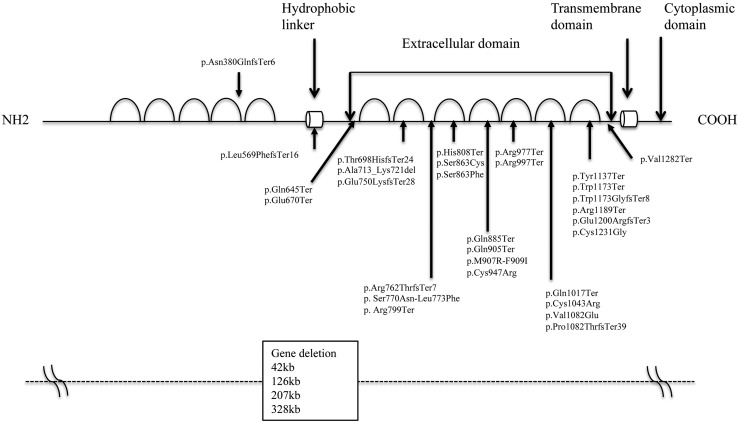
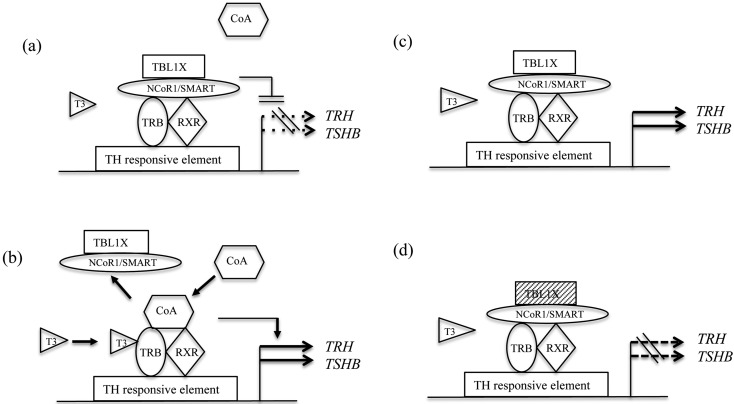
Congenital central hypothyroidism (C-CH) is caused by defects in the secretion of thyrotropin-releasing hormone (TRH) and/or TSH, leading to an impairment in the release of hormones from the thyroid. The causes of C-CH include congenital anomalies of the hypothalamic-pituitary regions and several genetic defects. In terms of endocrinology, C-CH is divided into two categories: (1) accompanied by another pituitary hormone deficiency and called combined pituitary hormone deficiency, and (2) isolated C-CH, showing mainly TSH deficiency. For isolated C-CH, a mutation in the TSH gene (TSHB) encoding the β-subunit of the protein was first found in 1990 by Japanese researchers, and thereafter several mutations in TSHB have been reported. Mutations in the thyrotropin-releasing hormone receptor gene (TRHR), as well as genetic defects in immunoglobulin superfamily 1 (IGSF1), have also been identified. It was recently found that isolated C-CH is caused by mutations in transducin β-like 1 X-linked and insulin receptor substrate 4. It is noted that all patients with TSHB deficiency and some with IGSF1 deficiency show severe hypothyroidism soon after birth. Among the causes of C-CH, high frequency of mutations in IGSF1 is the most prevalent. This review focuses on recent findings on isolated C-CH.
Keywords: TBL1X; TRHR; congenital central hypothyroidism (C-CH); immunoglobulin superfamily 1 (IGSF1).
Figures
Similar articles
-
Familial Central Hypothyroidism Caused by a Novel IGSF1 Gene Mutation.Thyroid. 2016 Dec;26(12):1693-1700. doi: 10.1089/thy.2015.0672. Epub 2016 Jul 25. Thyroid. 2016. PMID: 27310681
-
Genetics of Congenital Isolated TSH Deficiency: Mutation Screening of the Known Causative Genes and a Literature Review.J Clin Endocrinol Metab. 2019 Dec 1;104(12):6229-6237. doi: 10.1210/jc.2019-00657. J Clin Endocrinol Metab. 2019. PMID: 31504637
-
Clinical and molecular analyses of isolated central congenital hypothyroidism based on a survey conducted in Japan.Endocr J. 2024 May 23;71(5):471-480. doi: 10.1507/endocrj.EJ23-0391. Epub 2024 Mar 8. Endocr J. 2024. PMID: 38462462
-
Congenital isolated central hypothyroidism: Novel mutations and their functional implications.Handb Clin Neurol. 2021;180:161-169. doi: 10.1016/B978-0-12-820107-7.00010-0. Handb Clin Neurol. 2021. PMID: 34225927 Review.
-
Neonatal screening and a new cause of congenital central hypothyroidism.Ann Pediatr Endocrinol Metab. 2014 Sep;19(3):117-21. doi: 10.6065/apem.2014.19.3.117. Epub 2014 Sep 30. Ann Pediatr Endocrinol Metab. 2014. PMID: 25346914 Free PMC article. Review.
Cited by
-
A novel variant of IGSF1 in siblings with congenital central hypothyroidism whose diagnosis was prompted by school health checkups.Clin Pediatr Endocrinol. 2024;33(1):17-22. doi: 10.1297/cpe.2023-0046. Epub 2023 Nov 3. Clin Pediatr Endocrinol. 2024. PMID: 38299175 Free PMC article.
-
Imaging findings of thyroid diseases in children.Clin Pediatr Endocrinol. 2025 Apr;34(2):89-104. doi: 10.1297/cpe.2024-0082. Epub 2025 Jan 30. Clin Pediatr Endocrinol. 2025. PMID: 40201380 Free PMC article. Review.
-
Nuclear Receptor Coactivators (NCOAs) and Corepressors (NCORs) in the Brain.Endocrinology. 2020 Aug 1;161(8):bqaa083. doi: 10.1210/endocr/bqaa083. Endocrinology. 2020. PMID: 32449767 Free PMC article. Review.
-
A novel nonsense variant (p.Arg1293Ter) of the immunoglobulin superfamily 1 (IGSF1) associated with congenital hypogonadotropic hypogonadism and central hypothyroidism.Clin Pediatr Endocrinol. 2022;31(2):98-100. doi: 10.1297/cpe.2021-0071. Epub 2022 Jan 14. Clin Pediatr Endocrinol. 2022. PMID: 35431442 Free PMC article. No abstract available.
References
-
- Miyai K. Congenital thyrotropin deficiency--from discovery to molecular biology, postgenome and preventive medicine. Endocr J 2007;54: 191–203Review. doi: 10.1507/endocrj.KR-107 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous