

Percutaneous transorbital embolization of a carotid cavernous fistula
- PMID: 31384192
- PMCID: PMC6650229
- DOI: 10.1080/08998280.2019.1596502
Percutaneous transorbital embolization of a carotid cavernous fistula
Abstract
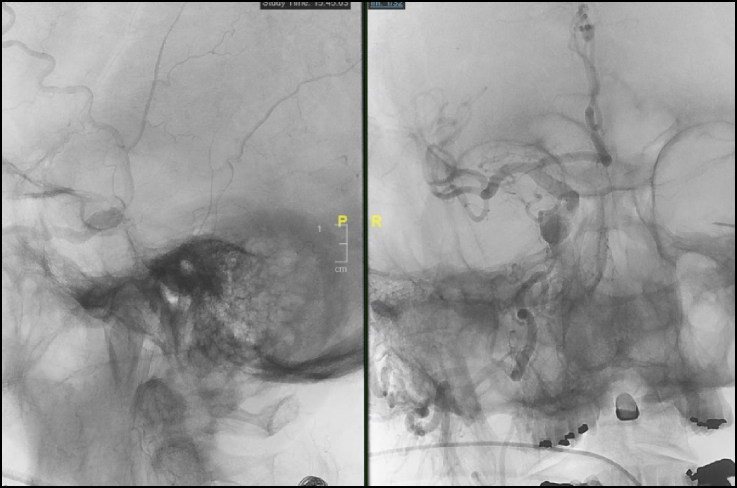
This case report highlights utilization of image-guided, percutaneous transorbital direct cavernous sinus puncture to embolize an anteriorly draining carotid cavernous fistula (CCF) when conventional transarterial and transvenous approaches were not feasible. An 86-year-old man with a known posterior draining CCF developed acute unilateral proptosis, pain, and vision loss ("red-eyed shunt"). Cerebral angiogram revealed the dural CCF to be draining anteriorly into partially thrombosed ophthalmic veins. After failed transarterial and transvenous attempts, a percutaneous transorbital approach was used to successfully embolize the fistula using the Onyx Liquid Embolic System according to the visual needle path generated by the Seimens Syngo iGuide. To our knowledge, this is the first reported case of percutaneous transorbital direct embolization of a CCF utilizing the Seimens Syngo iGuide.
Keywords: Carotid cavernous fistula; Seimens Syngo iGuide; onyx liquid embolic system; percutaneous transorbital direct cavernous sinus puncture.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources