

Case Reports
doi: 10.1080/08998280.2019.1617011.
eCollection 2019 Jul.
Mitral stenosis produced by infective endocarditis involving a previously anatomically normal valve
Affiliations
- PMID: 31384194
- PMCID: PMC6650209
- DOI: 10.1080/08998280.2019.1617011
Item in Clipboard
Case Reports
Mitral stenosis produced by infective endocarditis involving a previously anatomically normal valve
Proc (Bayl Univ Med Cent).
.
Abstract
Described herein is a 63-year-old man who developed methicillin-sensitive Staphylococcus aureus endocarditis on a previously anatomically normal mitral valve. The resulting vegetations were so large that severe mitral stenosis resulted. The development of valve stenosis due exclusively to infective endocarditis is extremely rare.
Keywords: Cerebral emboli; infective endocarditis; mitral stenosis; mitral valve replacement.
Figures
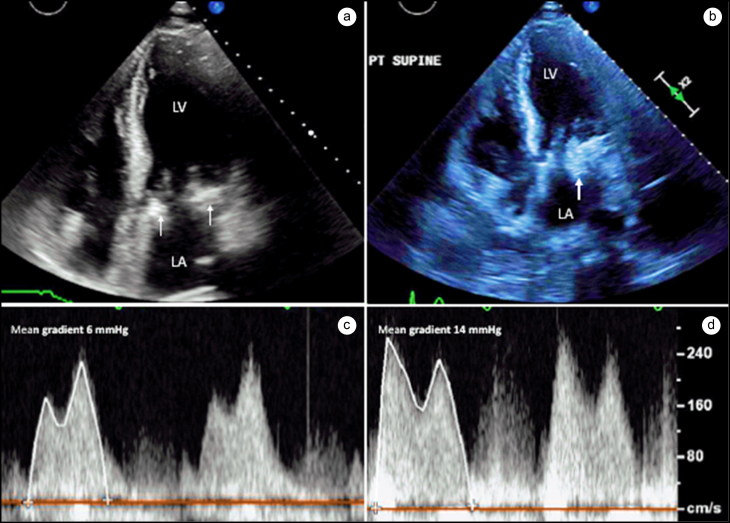
Four-chamber views from (a) initial study and (b) 1 month later. Mitral annular calcium (arrows) is present on the initial study, with no evidence of endocarditis. A large vegetation (large arrow) is seen 1 month later. (c) Continuous wave Doppler of mitral inflow showing a mean gradient of 6 mm Hg on initial study, (d) which increased to 14 mm Hg due to obstruction from the large vegetation.

Photographs of the entire operatively excised mitral valve (top) and close-up of the vegetation obstructing the mitral orifice. Scattered microorganisms, foci of polymorphonuclear and mononuclear cells, large collections of fibrin, and a few small calcific fragments were present histologically in the large vegetation.
References
Publication types
LinkOut - more resources
Full Text Sources