

Causes and risk factors for acute dialysis initiation among patients with end-stage kidney disease-a large retrospective observational cohort study
- PMID: 31384448
- PMCID: PMC6671523
- DOI: 10.1093/ckj/sfy118
Causes and risk factors for acute dialysis initiation among patients with end-stage kidney disease-a large retrospective observational cohort study
Abstract
Background: Patients who require acute initiation of dialysis have higher mortality rates when compared with patients with planned starts. Our primary objective was to explore the reasons and risk factors for acute initiation of renal replacement therapy (RRT) among patients with end-stage kidney disease (ESKD). Our secondary objective was to determine the difference in glomerular filtration rate (GFR) change in the year preceding RRT between elective and acute dialysis starts.
Methods: We conducted a single-centre retrospective observational study. ESKD patients either started dialysis electively (planned starters) or acutely and were known to renal services for >90 (unplanned starters) or <90 days (urgent starters).
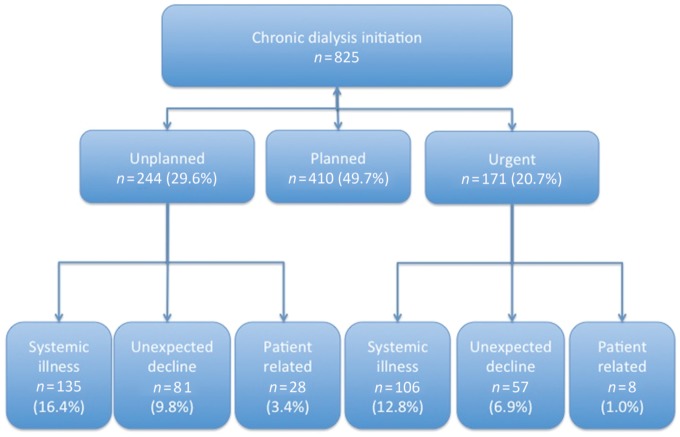
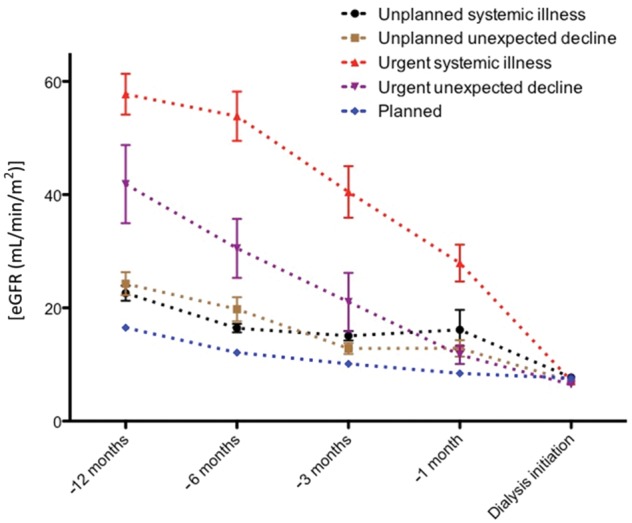
Results: In all, 825 consecutive patients initiated dialysis between January 2013 and December 2015. Of these, 410 (49.7%) patients had a planned start. A total of 415 (50.3%) patients had an acute start on dialysis: 244 (58.8%) unplanned and 171 (41.2%) urgent. The reasons for acute dialysis initiation included acute illness (58%) and unexplained decline to ESKD (33%). Cardiovascular disease [n = 30 (22%)] and sepsis [n = 65 (48%)] accounted for the majority of acute systemic illness. Age and premorbid cardiovascular disease were independent risk factors for acute systemic illness among unplanned starts, whereas autoimmune disease accounted for the majority of urgent starts. The rate of decline in GFR was greater in the month preceding RRT among acute dialysis starters compared with planned starters (P < 0.001).
Conclusions: Cardiovascular disease and advancing age were independent risk factors for emergency dialysis initiation among patients known to renal services for >3 months. The rapid and often unpredictable loss of renal function in the context of acute systemic illness poses a challenge to averting emergency dialysis start.
Keywords: acute dialysis start; renal replacement therapy; unplanned.
Figures
References
-
- Mendelssohn DC, Curtis B, Yeates K. et al. Suboptimal initiation of dialysis with and without early referral to a nephrologist. Nephrol Dial Transplant 2011; 26: 2959–2965 - PubMed
-
- Arora P, Obrador GT, Ruthazer R. et al. Prevalence, predictors, and consequences of late nephrology referral at a tertiary care center. J Am Soc Nephrol 1999; 10: 1281–1286 - PubMed
-
- Ifudu O, Dawood M, Homel P. et al. Excess morbidity in patients starting uremia therapy without prior care by a nephrologist. Am J Kidney Dis 1996; 28: 841–845 - PubMed
-
- Jungers P, Zingraff J, Albouze G. et al. Late referral to maintenance dialysis: detrimental consequences. Nephrol Dial Transplant 1993; 8: 1089–1093 - PubMed
LinkOut - more resources
Full Text Sources
