

Impact of wearable physical activity monitoring devices with exercise prescription or advice in the maintenance phase of cardiac rehabilitation: systematic review and meta-analysis
- PMID: 31384474
- PMCID: PMC6668165
- DOI: 10.1186/s13102-019-0126-8
Impact of wearable physical activity monitoring devices with exercise prescription or advice in the maintenance phase of cardiac rehabilitation: systematic review and meta-analysis
Abstract
Background: Physical activity (PA) is a component of cardiac rehabilitation (CR). However, life-long engagement in PA is required to maintain benefits gained. Wearable PA monitoring devices (WPAM) are thought to increase PA. There appear to be no reviews which investigate the effect of WPAM in cardiac populations. We firstly aimed to systematically review randomised controlled trials within the cardiac population that investigated the effect WPAM had through the maintenance phase of CR. We specifically examined the effect on cardiorespiratory fitness (CRF), amount and intensity of daily PA, and sedentary time. Secondly, we aimed to collate outcome measures reported, reasons for drop out, adverse events, and psychological impact from utilising a WPAM.
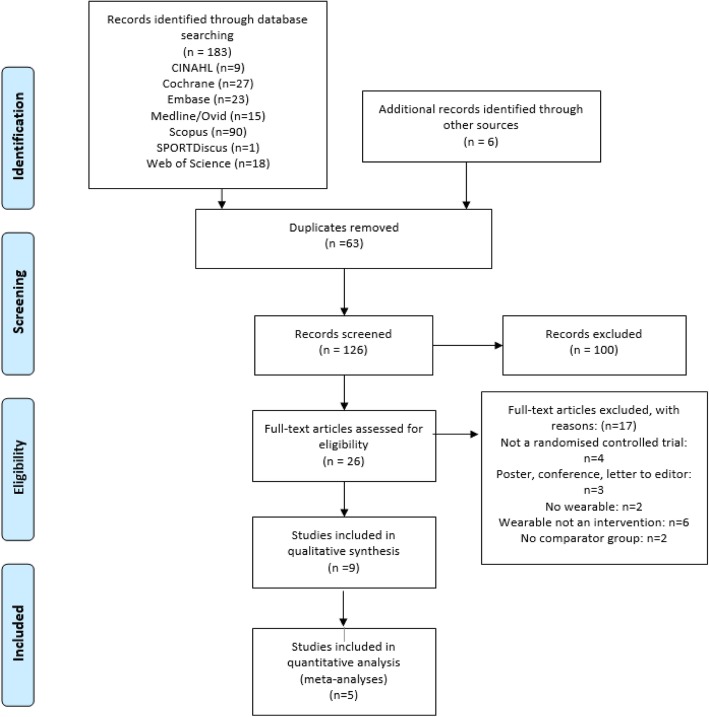
Methods: A systematic search (up to January 2019) of relevant databases was completed, followed by a narrative synthesis, meta-analysis and qualitative analysis.
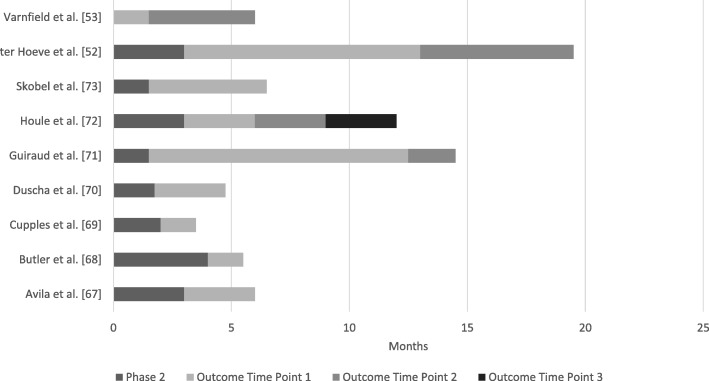
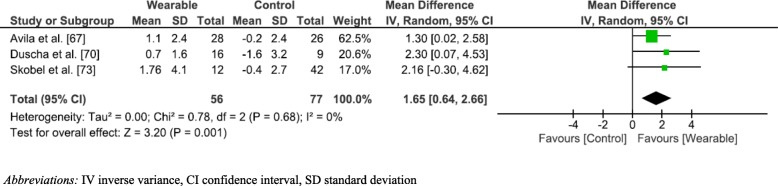
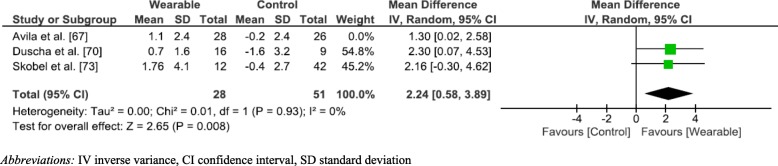
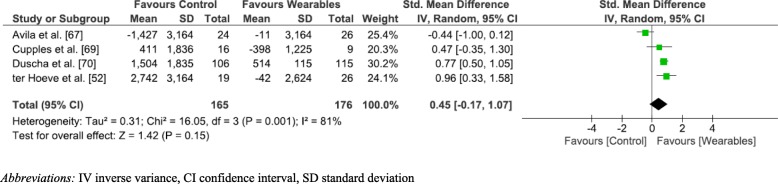
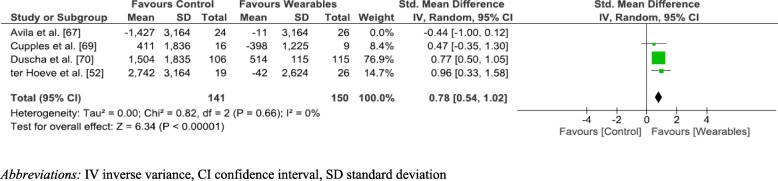
Results: Nine studies involving 1,352 participants were included. CRF was improved to a greater extent in participants using WPAM with exercise prescription or advice compared with controls (MD 1.65 mL/kg/min;95% confidence interval [CI; 0.64-2.66]; p = 0.001; I2 = 0%). There was no significant between group difference in six-minute walk test distance. In 70% of studies, step count was greater in participants using a WPAM with exercise prescription or advice, however the overall effect was not significant (SMD 0.45;95% [CI; - 0.17-1.07] p = 0.15; I2 = 81%). A sensitivity analysis resulted in significantly greater step counts in participants using a WPAM with exercise prescription or advice and reduced the heterogeneity from 81 to 0% (SMD 0.78;95% [CI;0.54-1.02]; p < 0.001; I2 = 0%). Three out of four studies reporting on intensity, found significantly increased time spent in moderate and moderate-vigorous intensity PA. No difference between groups was found for sedentary time. Three of six studies reported improved psychological benefits.No cardiac adverse events related to physical activity were reported and 62% of non-cardiac adverse events were primarily musculoskeletal injuries. Reasons for dropping out included medical conditions, lack of motivation, loss of interest, and technical difficulties.
Conclusions: Our meta-analysis showed WPAM with exercise prescription or advice are superior to no device in improving CRF in the maintenance phase of CR and no cardiac adverse events were reported with WPAM use. Our qualitative analysis showed evidence in favour of WPAM with exercise prescription or advice for both CRF and step count. WPAM with exercise prescription or advice did not change sedentary time. Psychological health and exercise intensity may potentially be enhanced by WPAM with exercise prescription or advice, however further research would strengthen this conclusion.
Trial registration: PROSPERO Registration Number: CRD42019106591.
Keywords: Cardiac rehabilitation; Cardiovascular disease; Coronary artery disease; Exercise; Maintenance phase; Wearable devices.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- Hamilton-Craig I. Secondary Prevention of Coronary Heart Disease. Med Today. 2009;10(1):36–44.
-
- Wood D, De backer G, Faergeman O, Graham I, Mancia G, Pyörälä K. Prevention of coronary heart disease in clinical practice: Recommendations of the Second Joint Task Force of European and other Societies on Coronary Prevention Second Joint Task Force of European and other Societies. Atherosclerosis. 1998;140(2):199-270. - PubMed
-
- National Heart Foundation of Australia [homepage on internet]. Secondary prevention of cardiovascular disease: A call to action to improve the health of Australians. 2010. Available from: https://www.heartfoundation.org.au/for-professionals/clinical-informatio.... Accessed 27 Feb 2019.
LinkOut - more resources
Full Text Sources
