

Dermoscopy of Inflammatory Dermatoses (Inflammoscopy): An Up-to-Date Overview
- PMID: 31384489
- PMCID: PMC6659598
- DOI: 10.5826/dpc.0903a01
Dermoscopy of Inflammatory Dermatoses (Inflammoscopy): An Up-to-Date Overview
Abstract
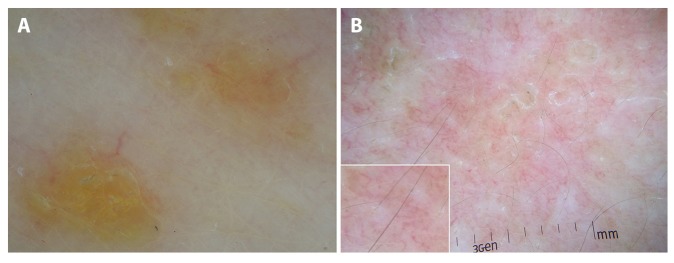
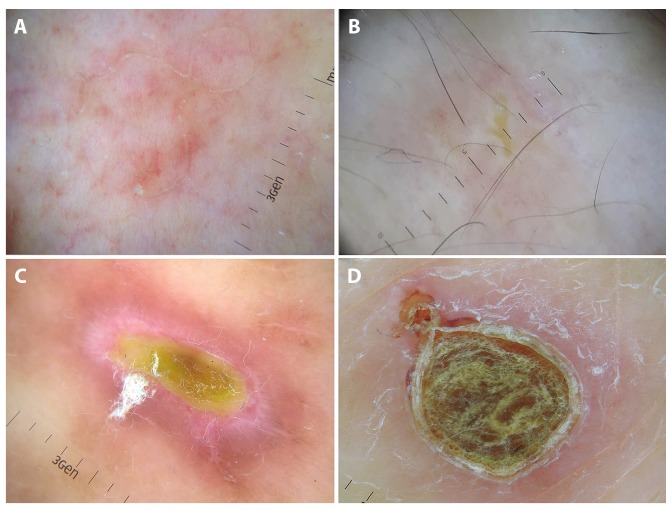
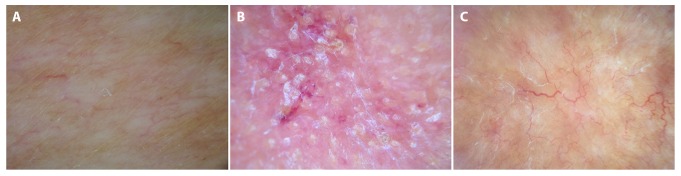
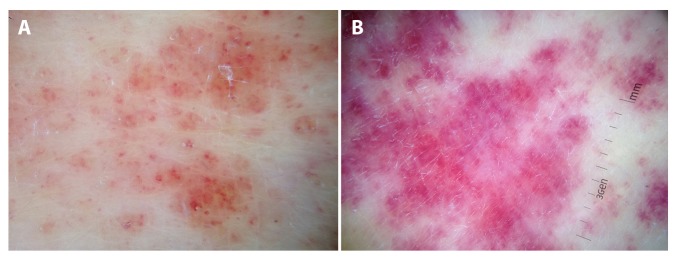
In addition to its use in pigmented and nonpigmented skin tumors, dermoscopy is gaining appreciation in assisting the diagnosis of nonneoplastic diseases, especially inflammatory dermatoses (inflammoscopy). In this field, dermoscopic examination should be considered as the second step of a "2-step procedure," always preceded by the establishment of a differential diagnosis on the basis of clinical examination. In this paper, we sought to provide an up-to-date overview on the use of dermoscopy in common inflammatory dermatoses based on the available literature data. For practical purposes, the analyzed dermatoses are grouped according to the clinical presentation pattern, in line with the 2-step procedure principle: erythematous-desquamative and papulosquamous dermatoses, papulokeratotic dermatoses, erythematous facial dermatoses, sclero-atrophic dermatoses, and miscellaneous.
Keywords: dermoscopy; differential diagnosis; general dermatology; inflammoscopy.
Conflict of interest statement
Competing interests: The author has no conflicts of interest to disclose.
Figures





References
-
- Errichetti E, Stinco G. The practical usefulness of dermoscopy in general dermatology. G Ital Dermatol Venereol. 2015;150(5):533–546. - PubMed
-
- Errichetti E, Zalaudek I, Kittler H, et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): an expert consensus on behalf of the International Dermoscopy Society. Br J Dermatol. 2019 May 11; doi: 10.1111/bjd.18125. Epub ahead of print. - DOI - PubMed
-
- Errichetti E, Stinco G. Clinical and dermoscopic response predictors in psoriatic patients undergoing narrowband ultraviolet B phototherapy: results from a prospective study. Int J Dermatol. 2018;57(6):681–686. - PubMed
-
- Lallas A, Kyrgidis A, Tzellos TG, et al. Accuracy of dermoscopic criteria for the diagnosis of psoriasis, dermatitis, lichen planus and pityriasis rosea. Br J Dermatol. 2012;166(6):1198–1205. - PubMed
LinkOut - more resources
Full Text Sources