

Triple-gated motion and blood pool clearance corrections improve reproducibility of coronary 18F-NaF PET
- PMID: 31385011
- PMCID: PMC6814554
- DOI: 10.1007/s00259-019-04437-x
Triple-gated motion and blood pool clearance corrections improve reproducibility of coronary 18F-NaF PET
Abstract
Purpose: To improve the test-retest reproducibility of coronary plaque 18F-sodium fluoride (18F-NaF) positron emission tomography (PET) uptake measurements.
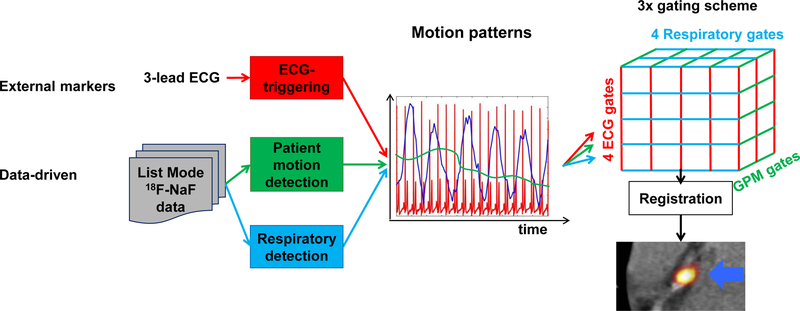
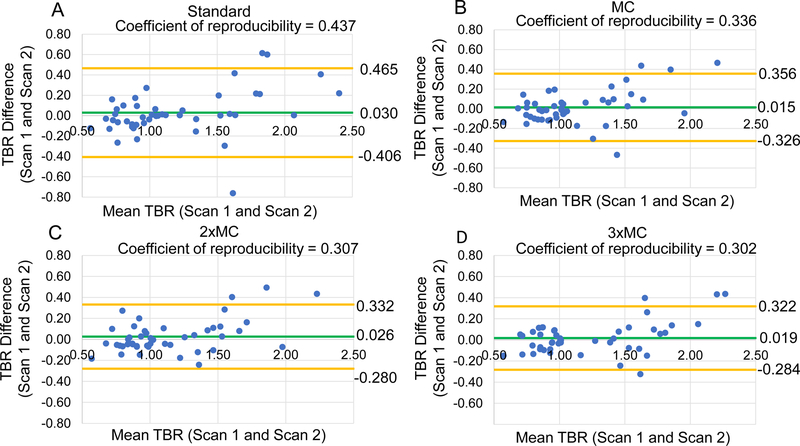
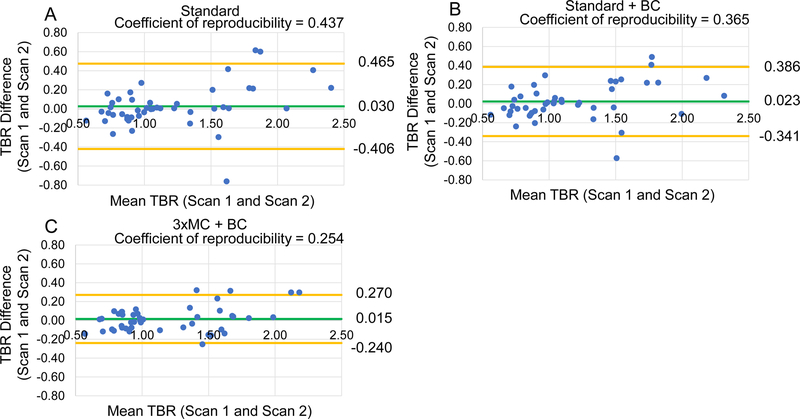
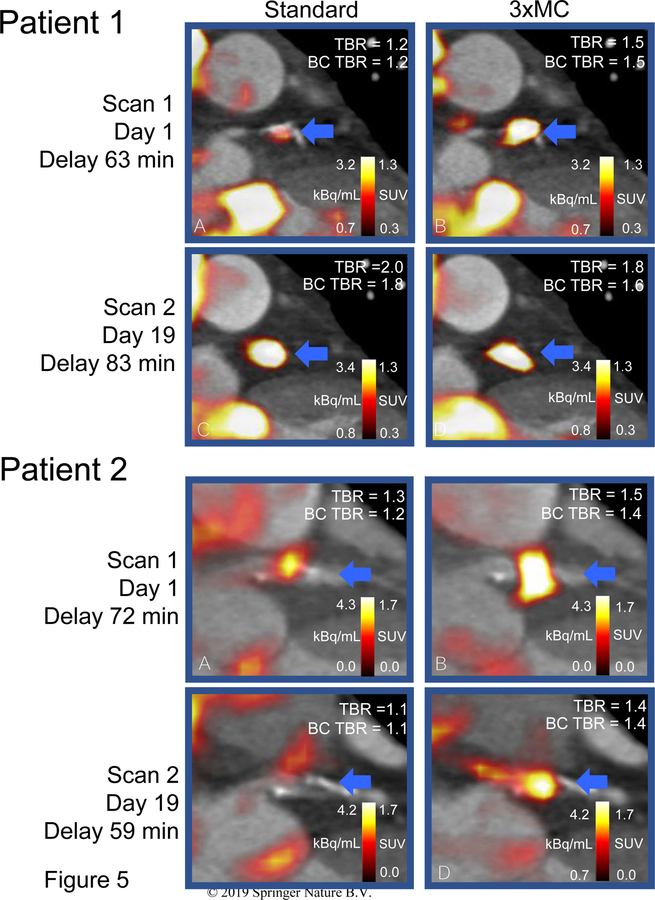
Methods: We recruited 20 patients with coronary artery disease who underwent repeated hybrid PET/CT angiography (CTA) imaging within 3 weeks. All patients had 30-min PET acquisition and CTA during a single imaging session. Five PET image-sets with progressive motion correction were reconstructed: (i) a static dataset (no-MC), (ii) end-diastolic PET (standard), (iii) cardiac motion corrected (MC), (iv) combined cardiac and gross patient motion corrected (2 × MC) and, (v) cardiorespiratory and gross patient motion corrected (3 × MC). In addition to motion correction, all datasets were corrected for variations in the background activities which are introduced by variations in the injection-to-scan delays (background blood pool clearance correction, BC). Test-retest reproducibility of PET target-to-background ratio (TBR) was assessed by Bland-Altman analysis and coefficient of reproducibility.
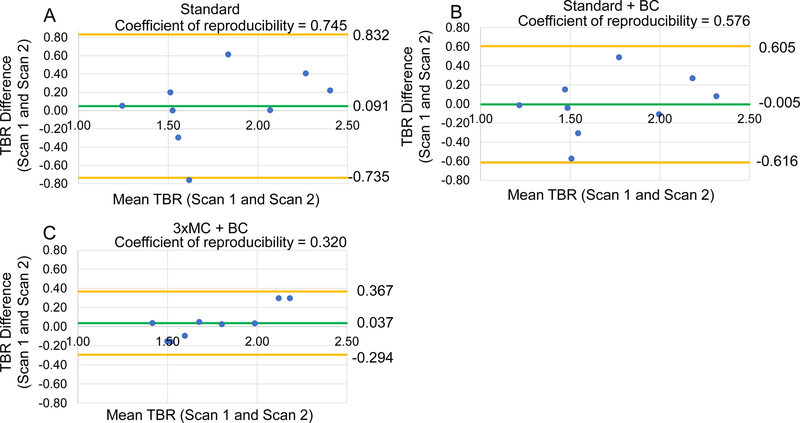
Results: A total of 47 unique coronary lesions were identified on CTA. Motion correction in combination with BC improved the PET TBR test-retest reproducibility for all lesions (coefficient of reproducibility: standard = 0.437, no-MC = 0.345 (27% improvement), standard + BC = 0.365 (20% improvement), no-MC + BC = 0.341 (27% improvement), MC + BC = 0.288 (52% improvement), 2 × MC + BC = 0.278 (57% improvement) and 3 × C + BC = 0.254 (72% improvement), all p < 0.001). Importantly, in a sub-analysis of 18F-NaF-avid lesions with gross patient motion > 10 mm following corrections, reproducibility was improved by 133% (coefficient of reproducibility: standard = 0.745, 3 × MC = 0.320).
Conclusion: Joint corrections for cardiac, respiratory, and gross patient motion in combination with background blood pool corrections markedly improve test-retest reproducibility of coronary 18F-NaF PET.
Keywords: 18F-sodium fluoride; Cardiac PET; Data-driven motion detection; Motion correction; PET/CT; Vulnerable plaque.
Figures
References
-
- Joshi NV, Vesey AT, Williams MC, Shah AS V, Calvert PA, Craighead FHM, et al. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: a prospective clinical trial. Lancet [Internet] Joshi et al. Open Access article distributed under the terms of CC BY; 2014;383:705–13. Available from: 10.1016/S0140-6736(13)61754-7 - DOI - PubMed
-
- Cocker MS, Spence JD, Hammond R, Wells G, DeKemp RA, Lum C, et al. [18F]-NaF PET/CT identifies active calcification in carotid plaque. JACC Cardiovasc Imaging 2017;10:486–8. - PubMed
-
- Rudd JHF, Warburton EA, Fryer TD, Jones HA, Clark JC, Antoun N, et al. Imaging atherosclerotic plaque inflammation with [18F]-fluorodeoxyglucose positron emission tomography. Circulation 2002;105:2708–11. - PubMed
-
- Dawood M, Büther F, Stegger L, Jiang X, Schober O, Schäfers M, et al. Optimal number of respiratory gates in positron emission tomography: a cardiac patient study. Med Phys [Internet] 2009;36:1775–84. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19544796 - PubMed
