

The Charcot foot: a pictorial review
- PMID: 31385060
- PMCID: PMC6682845
- DOI: 10.1186/s13244-019-0768-9
The Charcot foot: a pictorial review
Abstract
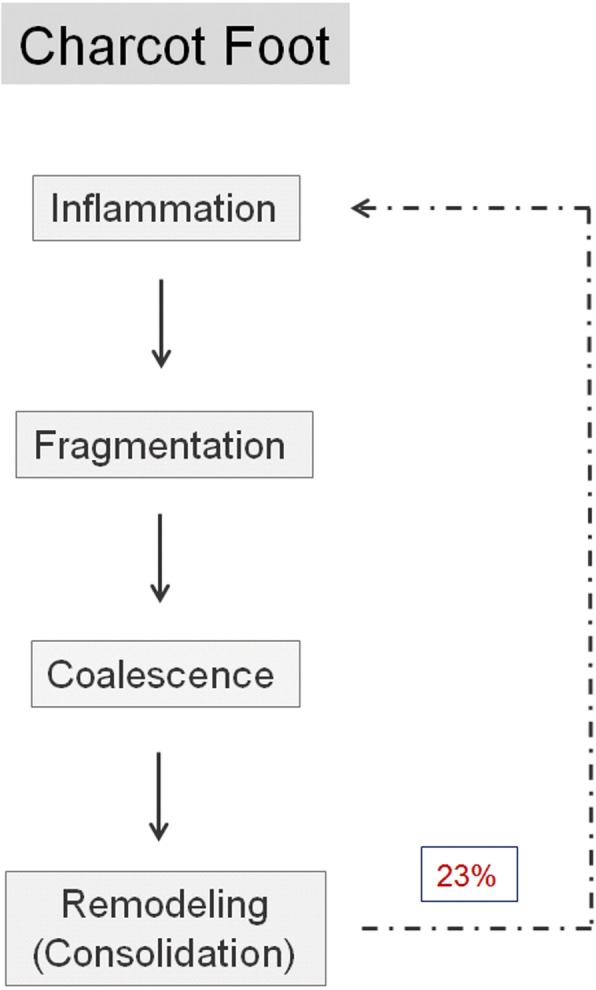
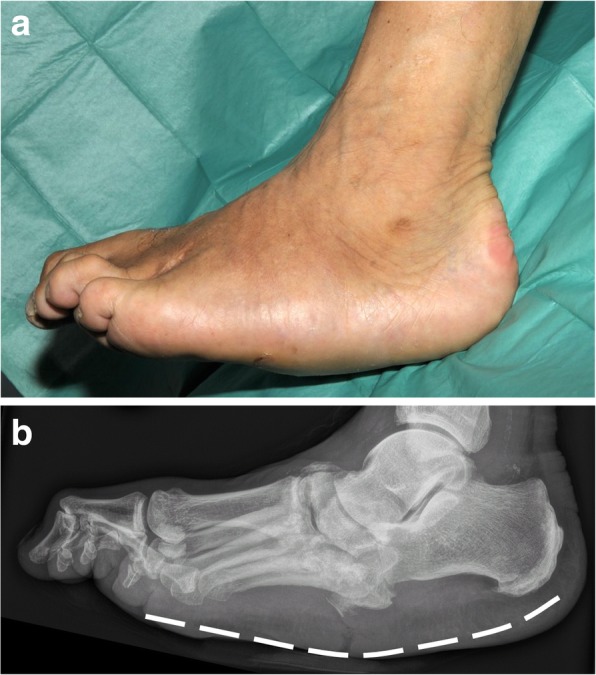
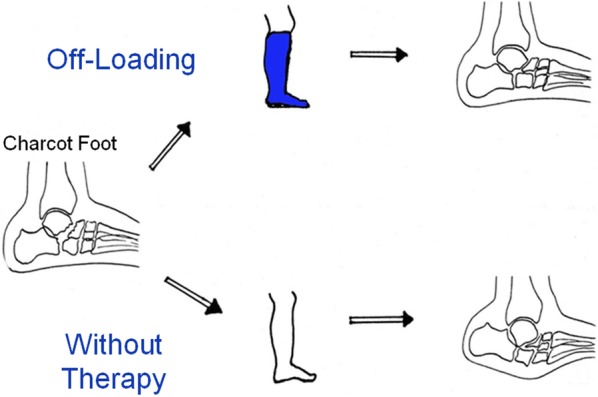
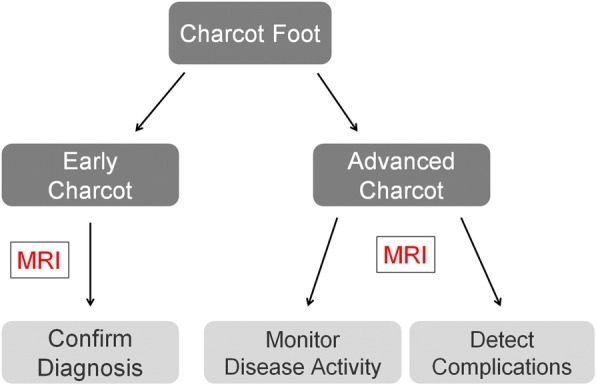
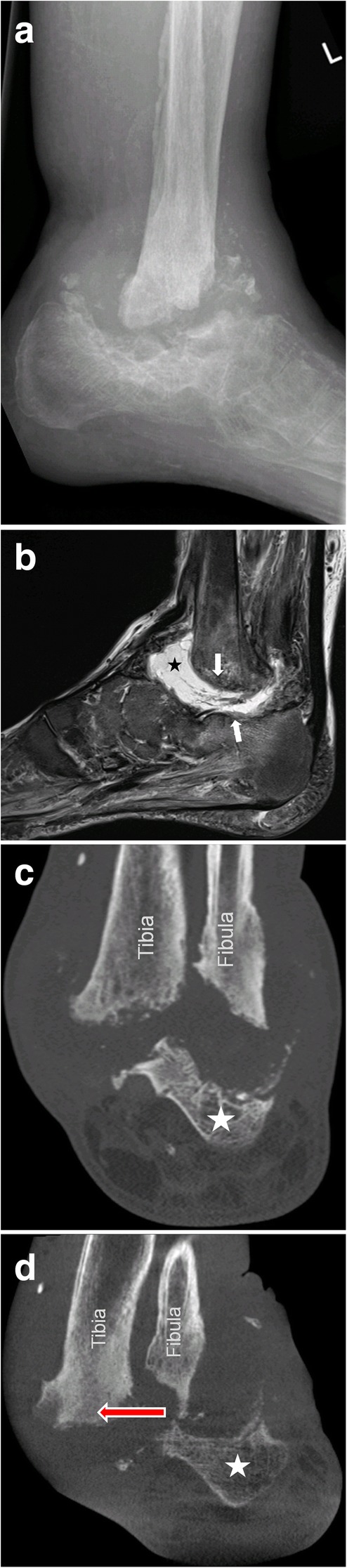
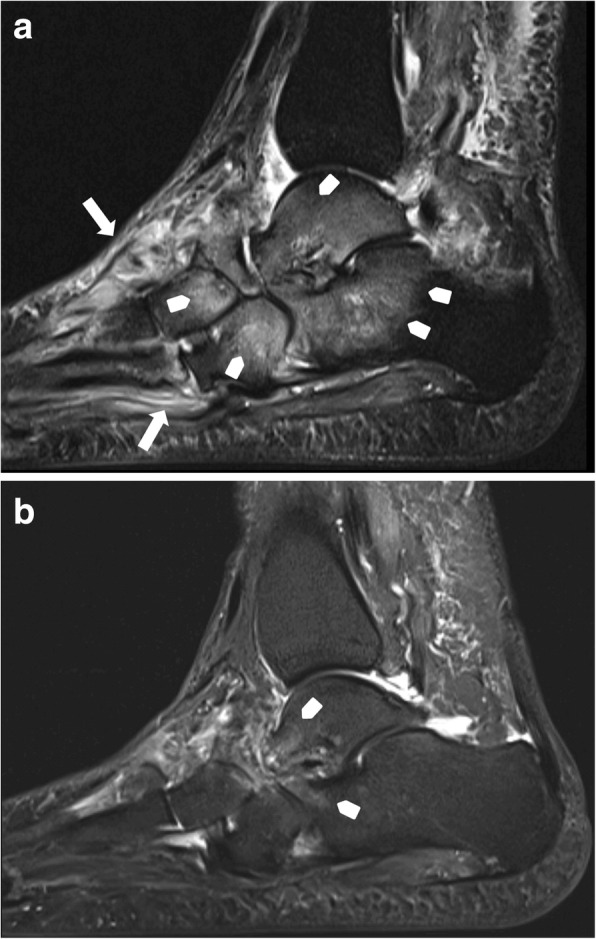
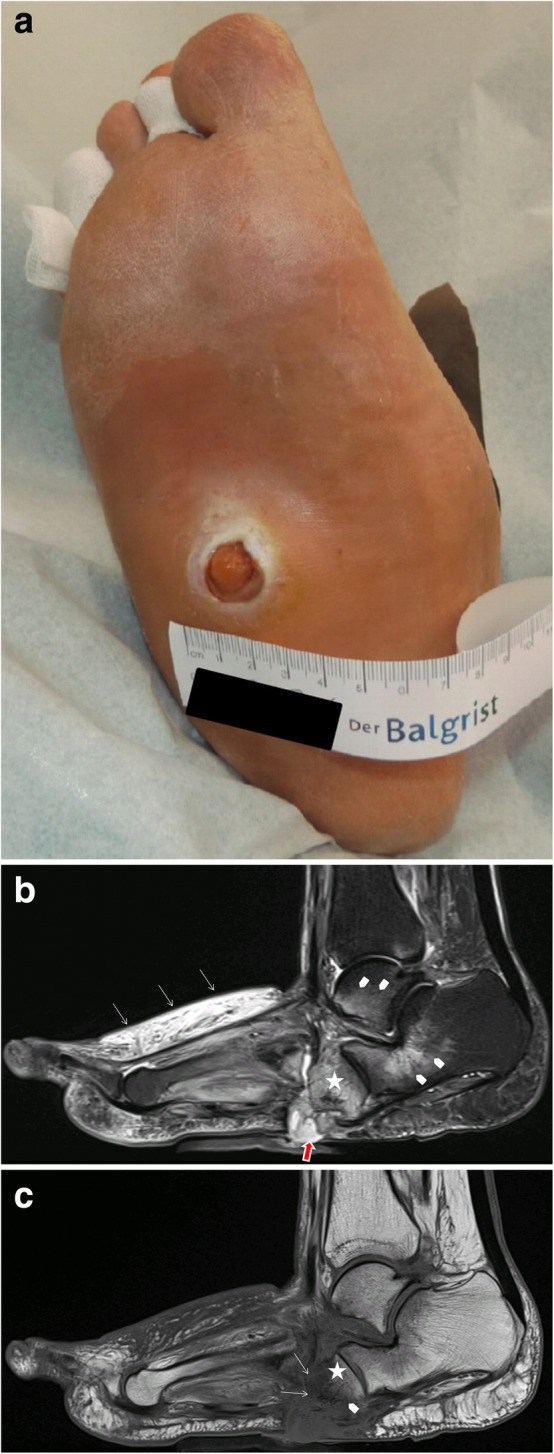
Charcot foot refers to an inflammatory pedal disease based on polyneuropathy; the detailed pathomechanism of the disease is still unclear. Since the most common cause of polyneuropathy in industrialized countries is diabetes mellitus, the prevalence in this risk group is very high, up to 35%. Patients with Charcot foot typically present in their fifties or sixties and most of them have had diabetes mellitus for at least 10 years. If left untreated, the disease leads to massive foot deformation. This review discusses the typical course of Charcot foot disease including radiographic and MR imaging findings for diagnosis, treatment, and detection of complications.
Keywords: Charcot foot; Imaging; MRI; Osteomyelitis; Radiographs.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Eichenholtz SN (1966) Charcot Joints. Charles C Thomas, Springfield, III, pp. 3–10
Publication types
LinkOut - more resources
Full Text Sources
