

Acute care in glioblastoma: the burden and the consequences
- PMID: 31385967
- PMCID: PMC6655395
- DOI: 10.1093/nop/npw032
Acute care in glioblastoma: the burden and the consequences
Abstract
Background: The utilization of inpatient medical services by patients with glioblastoma (GBM) is not well studied. We sought to describe causes, frequency, and outcomes of acute care visits in GBM.
Methods: We conducted a retrospective study of 158 GBM patients at the University of Rochester over 5 years. Electronic medical records were reviewed to identify all local and outside acute care visits. Acute care visits were defined as any encounter resulting in an emergency department visit or inpatient admission.
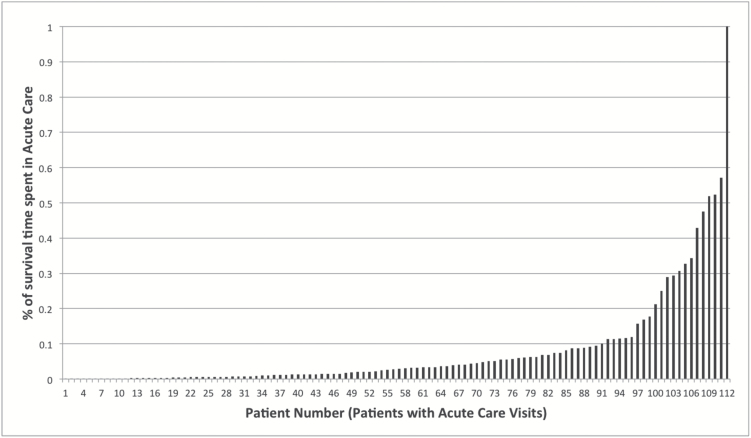
Results: Seventy-one percent (112/158) of GBM patients had 235 acute care visits corresponding to 163 hospitalizations (69%) and 72 emergency department visits (31%). Sixty-three percent of patients had multiple visits. Admission diagnoses were seizure (33%), neurosurgical procedure (15%), infection (12%), focal neurologic symptoms (9%), and venous thromboembolism (VTE, 9%). Forty-six patients had 1 or more visits for seizures. Median time to first acute care visit was 65.6 days and 22% of patients had an acute care visit within 30 days of diagnosis. Median length of stay was 5 days. Thirty-five percent of admitted patients were discharged home; 62% required a higher level of care than prior to admission (23% were discharged home with services, 17% to a nursing facility, 16% to hospice, 6% to acute rehab) and 3% died. Thirty-eight percent of patients had ACV within 30 days of death. Median survival was 14 months for patients who had acute care visits and 22.2 months for patients who did not.
Conclusion: The majority of GBM patients utilize acute care, most commonly for seizures. The high number of emergency department visits, short length of stay, and many patients discharged home suggest that some acute care visits may be avoidable.
Keywords: glioblastoma; health services; neuro-oncology; palliative care; seizures.
Figures



References
-
- Heimans JJ, Taphoorn MJ. Impact of brain tumour treatment on quality of life. J Neurol. 2002;249(8):955–960. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Stupp R, Taillibert S, Kanner AA, et al. maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. 2015;314(23):2535–2543. - PubMed
