

Outcomes of stereotactic radiosurgery of brain metastases from neuroendocrine tumors
- PMID: 31385968
- PMCID: PMC6655365
- DOI: 10.1093/nop/npx009
Outcomes of stereotactic radiosurgery of brain metastases from neuroendocrine tumors
Abstract
Background: Stereotactic radiosurgery (SRS) is an established treatment for brain metastases, yet little is known about SRS for neuroendocrine tumors given their unique natural history.
Objective: To determine outcomes and toxicity from SRS in patients with brain metastases arising from neuroendocrine tumors.
Methods: Thirty-three patients with brain metastases from neuroendocrine tumors who underwent SRS were retrospectively reviewed. Median age was 61 years and median Karnofsky performance status was 80. Primary sites were lung (87.9%), cervix (6.1%), esophagus (3%), and prostate (3%). Ten patients (30.3%) received upfront SRS, 7 of whom had neuroendocrine tumors other than small cell lung carcinoma. Kaplan-Meier survival and Cox regression analyses were performed to determine prognostic factors for survival.
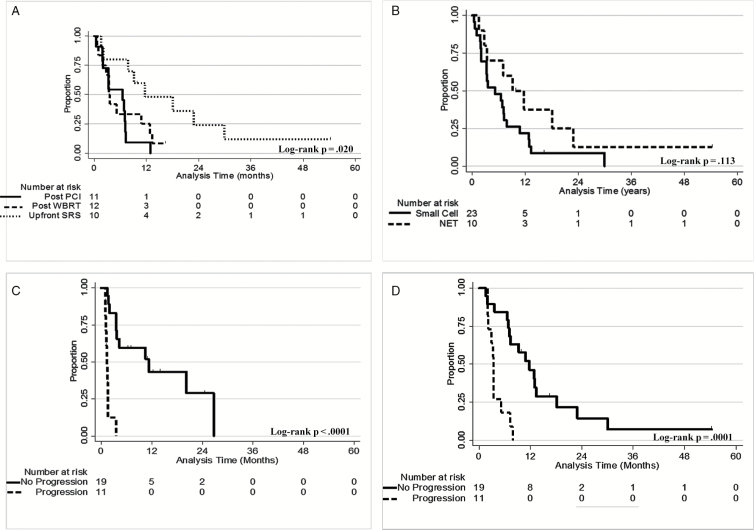
Results: With median follow-up after SRS of 5.3 months, local and distant brain recurrence developed in 5 patients (16.7%) and 20 patients (66.7%), respectively. Median overall survival (OS) after SRS was 6.9 months. Patients with progressive disease per Response Assessment in Neuro-Oncology-Brain Metastases (RANO-BM) criteria at 4 to 6 weeks after SRS had shorter median time to developing recurrence at a distant site in the brain and shorter OS than patients without progressive disease: 1.4 months and 3.3 months vs 11.4 months and 12 months, respectively (both P < .001). Toxicity was more likely in lesions of small cell histology than in lesions of other neuroendocrine tumor histology, 15.7% vs 3.3% (P = .021). No cases of grade 3 to 5 necrosis occurred.
Conclusions: SRS is an effective treatment option for patients with brain metastases from neuroendocrine tumors with excellent local control despite slightly higher toxicity rates than expected. Progressive disease at 4 to 6 weeks after SRS portends a poor prognosis.
Keywords: Gamma Knife; brain metastases; neuroendocrine; small cell carcinoma; stereotactic radiosurgery.
Figures
Similar articles
-
Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases.J Neurosurg. 2015 Nov;123(5):1261-7. doi: 10.3171/2014.12.JNS141919. Epub 2015 Jul 3. J Neurosurg. 2015. PMID: 26140482
-
Upfront stereotactic radiosurgery in patients with brain metastases from small cell lung cancer: retrospective analysis of 41 patients.Radiat Oncol. 2014 Jul 8;9:152. doi: 10.1186/1748-717X-9-152. Radiat Oncol. 2014. PMID: 25005424 Free PMC article.
-
Impact of 2-staged stereotactic radiosurgery for treatment of brain metastases ≥ 2 cm.J Neurosurg. 2018 Aug;129(2):366-382. doi: 10.3171/2017.3.JNS162532. Epub 2017 Sep 22. J Neurosurg. 2018. PMID: 28937324
-
Stereotactic radiosurgery for pancreatic neuroendocrine tumor brain Metastases: Systematic review and Illustrative case presentation.J Clin Neurosci. 2024 Dec;130:110927. doi: 10.1016/j.jocn.2024.110927. Epub 2024 Nov 20. J Clin Neurosci. 2024. PMID: 39571478
-
Is upfront stereotactic radiosurgery a rational treatment option for very elderly patients with brain metastases? A retrospective analysis of 106 consecutive patients age 80 years and older.BMC Cancer. 2016 Dec 15;16(1):948. doi: 10.1186/s12885-016-2983-9. BMC Cancer. 2016. PMID: 27978813 Free PMC article.
Cited by
-
Successful salvage of recurrent leptomeningeal disease in large cell neuroendocrine lung cancer with stereotactic radiotherapy.Strahlenther Onkol. 2021 Dec;197(12):1143-1147. doi: 10.1007/s00066-021-01814-0. Epub 2021 Aug 30. Strahlenther Onkol. 2021. PMID: 34459938 English.
-
Impact of metastasis site on overall survival in neuroendocrine cervical carcinoma.Abdom Radiol (NY). 2025 Jun;50(6):2703-2709. doi: 10.1007/s00261-024-04716-8. Epub 2024 Nov 27. Abdom Radiol (NY). 2025. PMID: 39592479 No abstract available.
-
Two case reports of brain metastases in patients with pancreatobiliary neuroendocrine carcinoma.Clin J Gastroenterol. 2021 Feb;14(1):386-390. doi: 10.1007/s12328-020-01270-w. Epub 2020 Oct 23. Clin J Gastroenterol. 2021. PMID: 33095423
References
-
- Klimstra DS, Modlin IR, Coppola D, et al. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010;39(6):707–712. - PubMed
-
- Rekhtman N. Neuroendocrine tumors of the lung: an update. Arch Pathol Lab Med. 2010;134(11):1628–1638. - PubMed
-
- Pamela K. Carcinoid and neuroendocrine tumors: building on success. J Clin Oncol. 2015;33(16):1855–1863. - PubMed
-
- Walenkamp AM, Sonke GS, Sleijfer DT. Clinical and therapeutic aspects of extrapulmonary small cell carcinoma. Cancer Treat Rev. 2009;35(3):228–236. - PubMed
-
- Maiuri F, Cappabianca P, Del Basso De Caro M, et al. Single brain metastases of carcinoid tumors. J Neurooncol. 2004;66(3):327–332. - PubMed
