

Treatment and survival differences across tumor sites in malignant peripheral nerve sheath tumors: a SEER database analysis and review of the literature
- PMID: 31386019
- PMCID: PMC6656331
- DOI: 10.1093/nop/npy025
Treatment and survival differences across tumor sites in malignant peripheral nerve sheath tumors: a SEER database analysis and review of the literature
Abstract
Background: Currently, literature is scarce on differences across all possible tumor sites in malignant peripheral nerve sheath tumors (MPNSTs). To determine differences in treatment and survival across tumor sites and assess possible predictors for survival, we used the Surveillance, Epidemiology, and End Results (SEER) database.
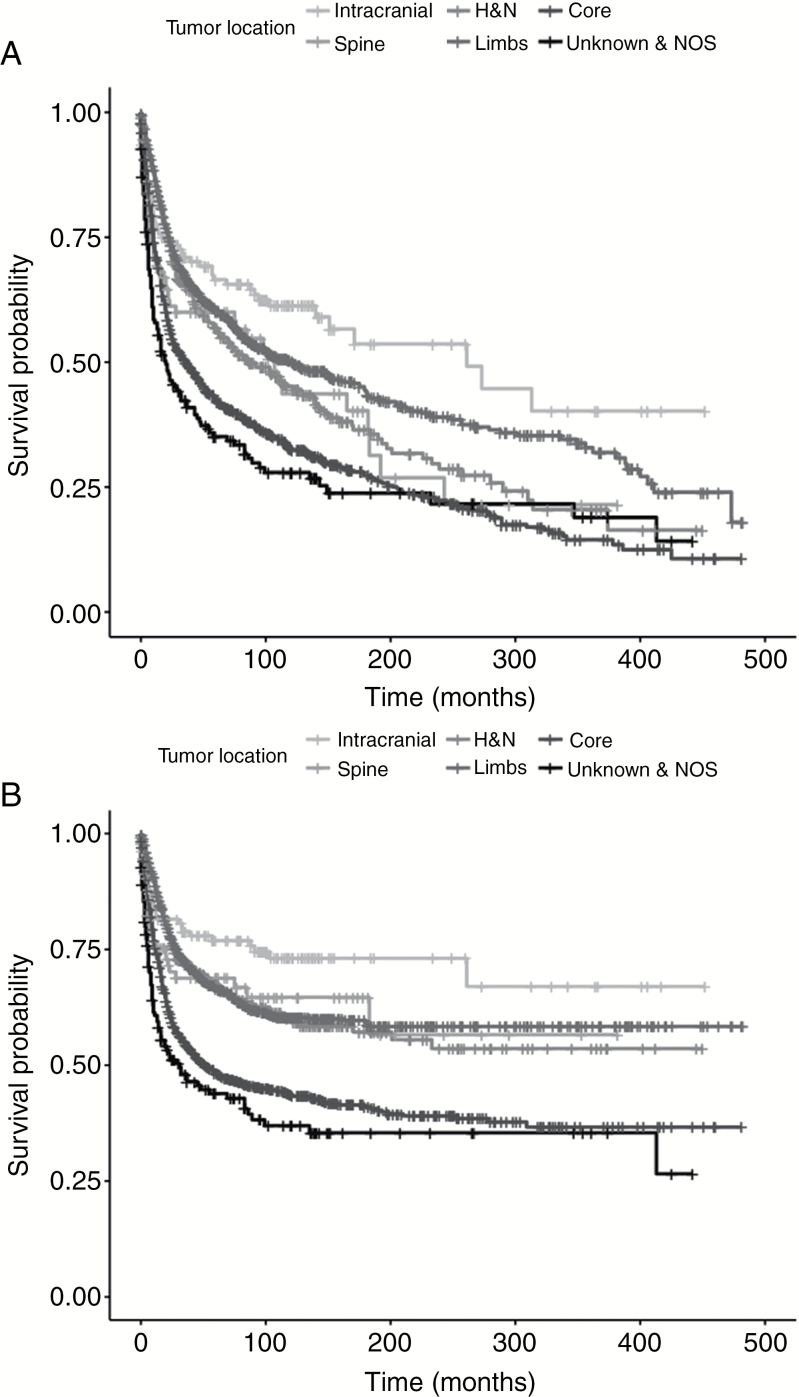
Methods: MPNST cases were obtained from the SEER database. Tumor sites were recoded into: intracranial, spinal, head and neck (H&N), limbs, core (thorax/abdomen/pelvis), and unknown site of origin. Patient and tumor characteristics, treatment modalities, and survival were extracted. Overall survival (OS) was assessed using univariable and multivariable Cox regression hazard models. Kaplan-Meier survival curves were constructed per tumor site for OS and disease-specific survival (DSS).
Results: A total of 3267 MPNST patients were registered from 1973 to 2013; 167 intracranial (5.1%), 119 spinal (3.6%), 449 H&N (13.7%), 1022 limb (31.3%), 1307 core (40.0%), and 203 unknown (6.2%). The largest tumors were found in core sites (80.0 mm, interquartile range [IQR]: 60.0-115.0 mm) and the smallest were intracranial (37.4 mm, IQR: 17.3-43.5 mm). Intracranial tumors were least frequently resected (58.1%), whereas spinal tumors were most often resected (83.0%). Radiation was administered in 35.5% to 41.8%. Independent factors associated with decreased survival were: older age, male sex, black race, no surgery, partial resection, large tumor size, high tumor grade, H&N site, and core site (all P < .05). Intracranial and pediatric tumors show superior survival (both P < .05). Intracranial tumors show superior OS and DSS curves, whereas core tumors have the worst (P < .001).
Conclusion: Superior survival is seen in intracranial and pediatric MPNSTs. Core and H&N tumors have a worse prognosis.
Keywords: MPNST; SEER; malignant peripheral nerve sheath tumor; survival; tumor site.
Figures
References
-
- Vauthey JN, Woodruff JM, Brennan MF. Extremity malignant peripheral nerve sheath tumors (neurogenic sarcomas): a 10-year experience. Ann Surg Oncol. 1995;2(2):126–131. - PubMed
-
- Ng VY, Scharschmidt TJ, Mayerson JL, Fisher JL. Incidence and survival in sarcoma in the United States: a focus on musculoskeletal lesions. Anticancer Res. 2013;33(6):2597–2604. - PubMed
-
- Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM Ilstrup DM. Malignant peripheral nerve sheath tumors. A clinicopathologic study of 120 cases. Cancer. 1986;57(10):2006–2021. - PubMed
