

Case-based review: primary central nervous system lymphoma
- PMID: 31386044
- PMCID: PMC6656340
- DOI: 10.1093/nop/npw033
Case-based review: primary central nervous system lymphoma
Abstract
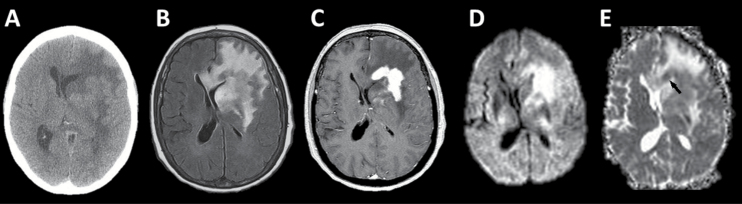
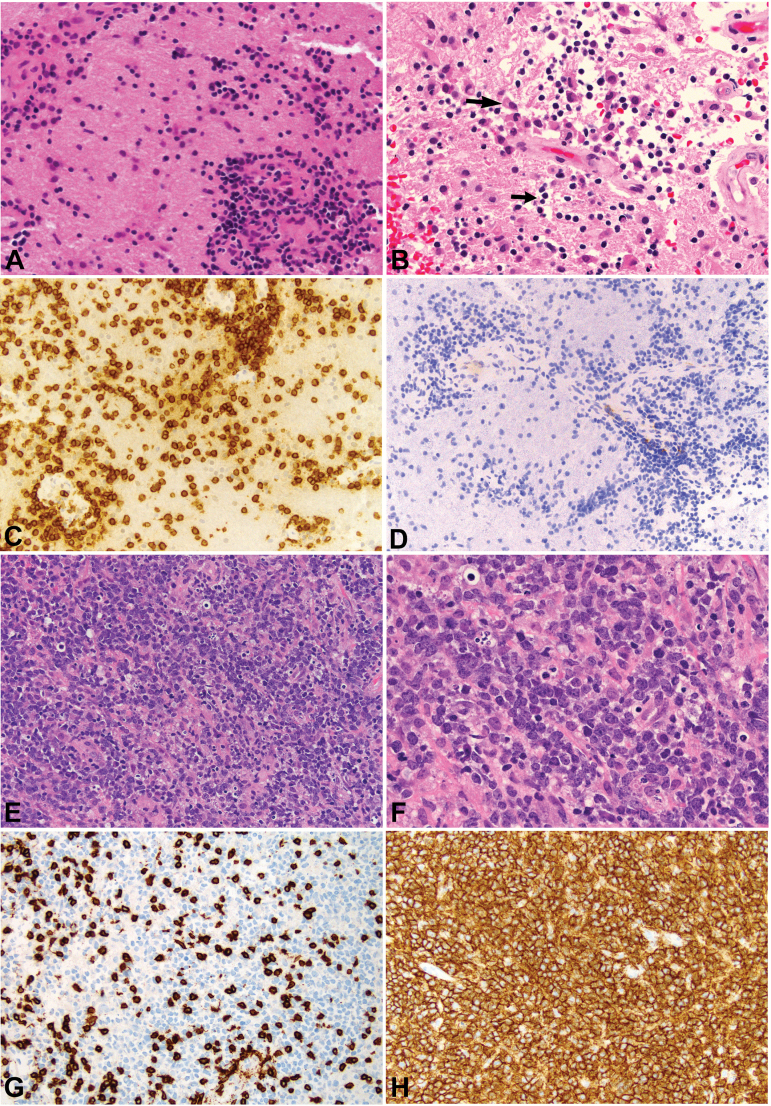
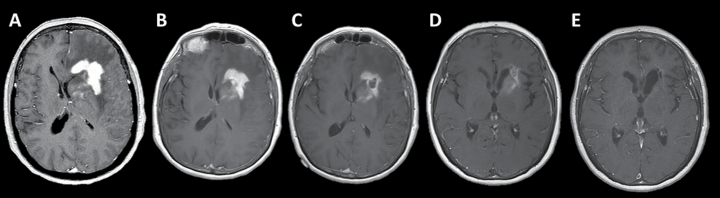
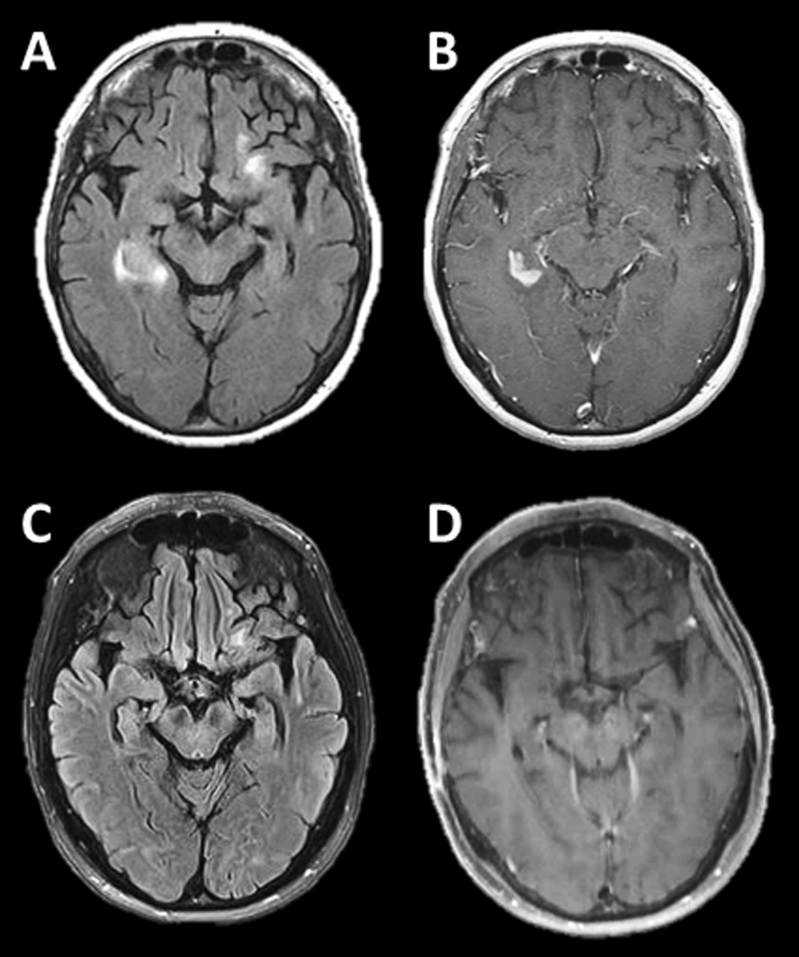
Primary CNS lymphoma (PCNSL) is a rare diffuse large B-cell lymphoma originating within the central nervous system. The overall incidence of PCNSL is rising, particularly in the elderly population. Immunosuppression is a strong risk factor, but most patients with this tumor are apparently immunocompetent. Diagnosis of PCNSL can be challenging. Non-invasive or minimally invasive tests such as ophthalmological evaluation and spinal fluid analysis may be useful, but the majority of patients require tumor biopsy for definitive diagnosis. Our knowledge concerning optimum treatment of PCNSL is fragmentary due to paucity of adequately sized trials. Most patients are now initially treated with high-dose-methotrexate-based chemotherapy alone, as the addition of whole-brain radiotherapy at standard doses has not been shown to increase survival and does increase the risk of neurological toxicity. Ongoing trials are addressing issues such as the roles of reduced-dose radiotherapy, the addition of the CD20 antibody rituximab to chemotherapy, high-dose chemotherapy followed by autologous stem cell transplantation, and maintenance therapy in the primary management of PCNSL.
Keywords: high-dose methotrexate; neurotoxicity; primary CNS lymphoma; whole-brain radiotherapy.
Figures
Similar articles
-
Diagnosis and management of primary central nervous system lymphoma.Cancer. 2017 Nov 15;123(22):4314-4324. doi: 10.1002/cncr.30965. Epub 2017 Sep 26. Cancer. 2017. PMID: 28950405 Review.
-
High-dose chemotherapy and autologous stem cell transplant compared with conventional chemotherapy for consolidation in newly diagnosed primary CNS lymphoma--a randomized phase III trial (MATRix).BMC Cancer. 2016 Apr 21;16:282. doi: 10.1186/s12885-016-2311-4. BMC Cancer. 2016. PMID: 27098429 Free PMC article. Clinical Trial.
-
Diagnosis and treatment of primary CNS lymphoma.Nat Rev Neurol. 2013 Jun;9(6):317-27. doi: 10.1038/nrneurol.2013.83. Epub 2013 May 14. Nat Rev Neurol. 2013. PMID: 23670107 Review.
-
A focus on pharmacotherapy for primary central nervous system lymphoma.Expert Rev Hematol. 2015 Oct;8(5):559-62. doi: 10.1586/17474086.2015.1066672. Epub 2015 Jul 9. Expert Rev Hematol. 2015. PMID: 26159859
-
High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial.Lancet Oncol. 2010 Nov;11(11):1036-47. doi: 10.1016/S1470-2045(10)70229-1. Epub 2010 Oct 20. Lancet Oncol. 2010. PMID: 20970380 Clinical Trial.
Cited by
-
Diagnostics and treatment delay in primary central nervous system lymphoma: What the neurosurgeon should know.Acta Neurochir (Wien). 2024 Jun 11;166(1):261. doi: 10.1007/s00701-024-06138-3. Acta Neurochir (Wien). 2024. PMID: 38858236 Free PMC article. Review.
-
Primary large B-cell lymphoma of the central nervous system with positive NMDAR antibody: a case report.BMC Neurol. 2022 Aug 12;22(1):298. doi: 10.1186/s12883-022-02821-z. BMC Neurol. 2022. PMID: 35962342 Free PMC article.
-
A Rare Presentation of Primary Central Nervous System Lymphoma in an Immunocompetent Patient.Cureus. 2022 Apr 5;14(4):e23858. doi: 10.7759/cureus.23858. eCollection 2022 Apr. Cureus. 2022. PMID: 35530884 Free PMC article.
References
-
- Korfel A, Schlegel U. Diagnosis and treatment of primary CNS lymphoma. Nat Rev Neurol. 2013;9(6):317–327. - PubMed
-
- Porter AB, Giannini C, Kaufmann T, et al. Primary central nervous system lymphoma can be histologically diagnosed after previous corticosteroid use: a pilot study to determine whether corticosteroids prevent the diagnosis of primary central nervous system lymphoma. Ann Neurol. 2008;63(5):662–667. - PubMed
-
- Haldorsen IS, Espeland A, Larsen JL, et al. Diagnostic delay in primary central nervous system lymphoma. Acta Oncol. 2005;44(7):728–734. - PubMed
-
- Hoang-Xuan K, Bessell E, Bromberg J, et al. ; European Association for Neuro-Oncology Task Force on Primary CNS Lymphoma. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol. 2015;16(7):e322–e332. - PubMed
-
- Goldschmidt N, Linetsky E, Shalom E, et al. High incidence of thromboembolism in patients with central nervous system lymphoma. Cancer. 2003;98(6):1239–1242. - PubMed
