

Routinely reported ejection fraction and mortality in clinical practice: where does the nadir of risk lie?
- PMID: 31386109
- PMCID: PMC8204658
- DOI: 10.1093/eurheartj/ehz550
Routinely reported ejection fraction and mortality in clinical practice: where does the nadir of risk lie?
Abstract
Aims: We investigated the relationship between clinically assessed left ventricular ejection fraction (LVEF) and survival in a large, heterogeneous clinical cohort.
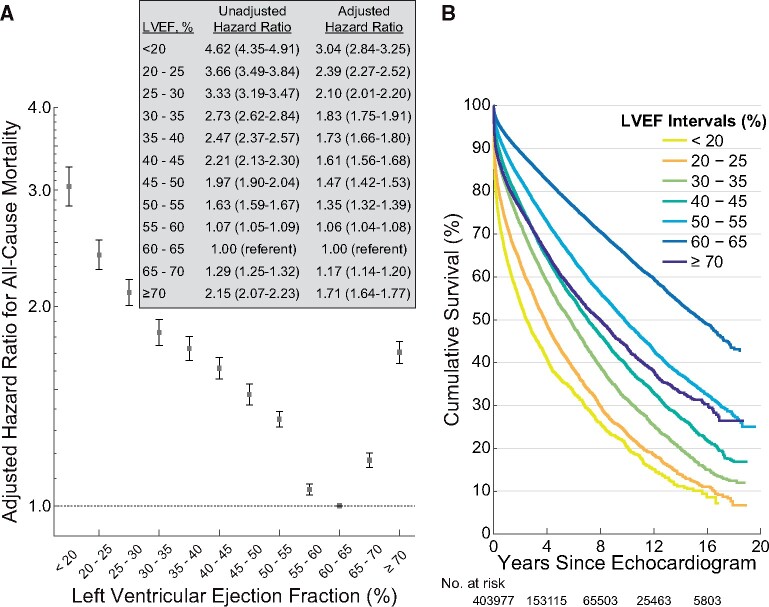
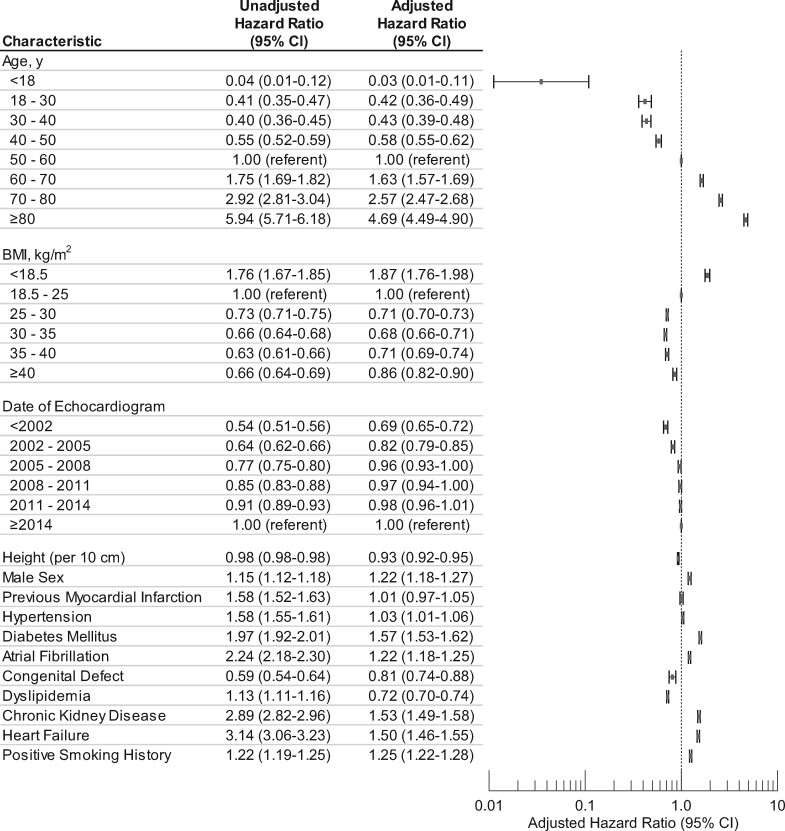
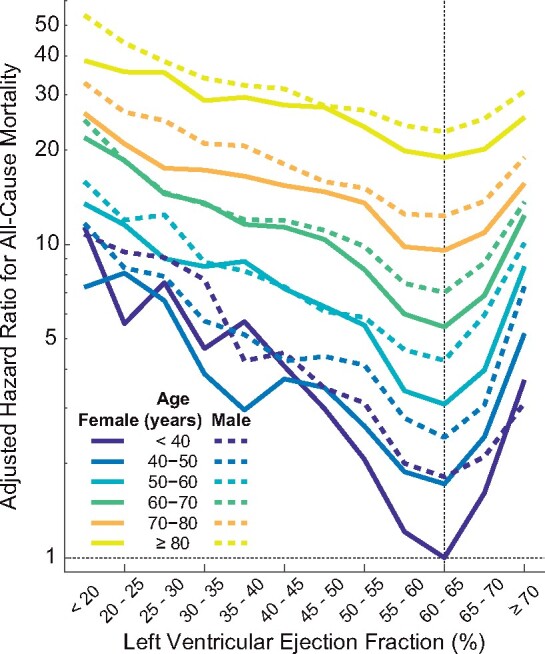
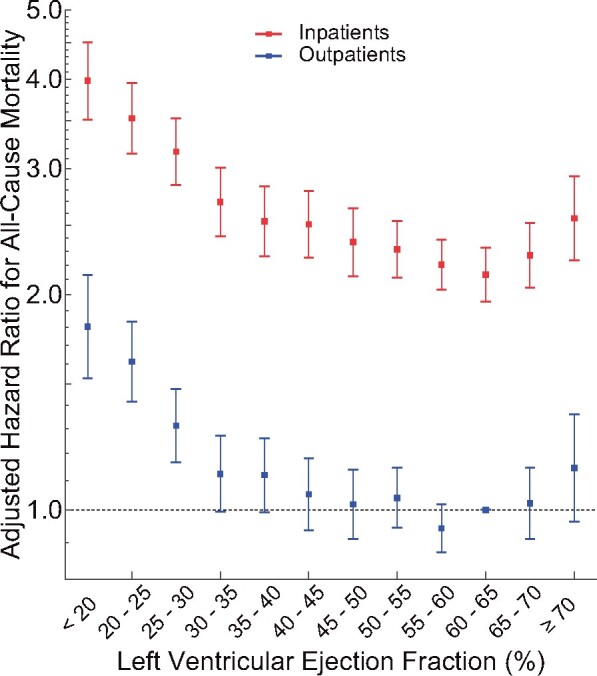
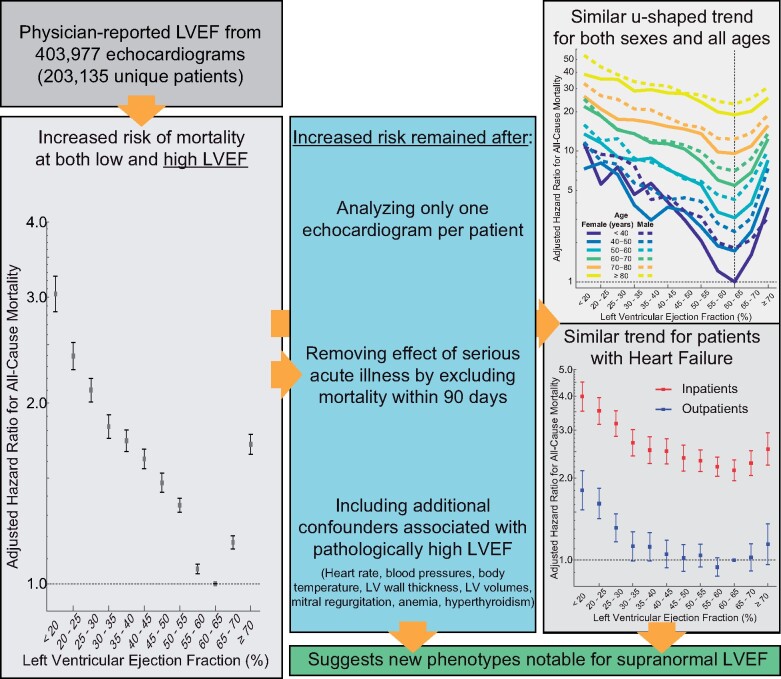
Methods and results: Physician-reported LVEF on 403 977 echocardiograms from 203 135 patients were linked to all-cause mortality using electronic health records (1998-2018) from US regional healthcare system. Cox proportional hazards regression was used for analyses while adjusting for many patient characteristics including age, sex, and relevant comorbidities. A dataset including 45 531 echocardiograms and 35 976 patients from New Zealand was used to provide independent validation of analyses. During follow-up of the US cohort, 46 258 (23%) patients who had undergone 108 578 (27%) echocardiograms died. Overall, adjusted hazard ratios (HR) for mortality showed a u-shaped relationship for LVEF with a nadir of risk at an LVEF of 60-65%, a HR of 1.71 [95% confidence interval (CI) 1.64-1.77] when ≥70% and a HR of 1.73 (95% CI 1.66-1.80) at LVEF of 35-40%. Similar relationships with a nadir at 60-65% were observed in the validation dataset as well as for each age group and both sexes. The results were similar after further adjustments for conditions associated with an elevated LVEF, including mitral regurgitation, increased wall thickness, and anaemia and when restricted to patients reported to have heart failure at the time of the echocardiogram.
Conclusion: Deviation of LVEF from 60% to 65% is associated with poorer survival regardless of age, sex, or other relevant comorbidities such as heart failure. These results may herald the recognition of a new phenotype characterized by supra-normal LVEF.
Keywords: Cardiac function; Clinical practice; Ejection fraction; Mortality; Survival.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2019. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Hyperdynamic left ventricular function and the prognostic implications for heart failure with preserved ejection fraction.Eur Heart J. 2020 Mar 21;41(12):1258-1259. doi: 10.1093/eurheartj/ehz706. Eur Heart J. 2020. PMID: 31651945 No abstract available.
References
-
- Virnig BA, Shippee ND, O’Donnell B, Zeglin J, Parashuram S. Trends in the Use of Echocardiography, 2007 to 2011. Echocardiography Trends. Data Points #20 (prepared by the University of Minnesota DEcIDE Center, under Contract No. HHSA29020100013I). Rockville, MD: Agency for Healthcare Research and Quality; May 2014. AHRQ Publication No. 14-EHC034-EF.
-
- Solomon SD, Anavekar N, Skali H, McMurray JJV, Swedberg K, Yusuf S, Granger CB, Michelson EL, Wang D, Pocock S, Pfeffer MA. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005;112:3738–3744. - PubMed
-
- Bart BA, Shaw LK, McCants CB, Fortin DF, Lee KL, Califf RM, O'Connor CM. Clinical determinants of mortality in patients with angiographically diagnosed ischemic or nonischemic cardiomyopathy. J Am Coll Cardiol 1997;30:1002–1008. - PubMed
-
- Giannuzzi P, Temporelli PL, Bosimini E, Silva P, Imparato A, Corrà U, Galli M, Giordano A. Independent and incremental prognostic value of Doppler-derived mitral deceleration time of early filling in both symptomatic and asymptomatic patients with left ventricular dysfunction. J Am Coll Cardiol 1996;28:383–390. - PubMed
-
- Juillière Y, Barbier G, Feldmann L, Grentzinger A, Danchin N, Cherrier F. Additional predictive value of both left and right ventricular ejection fractions on long-term survival in idiopathic dilated cardiomyopathy. Eur Heart J 1997;18:276–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
