

Association of Office and Ambulatory Blood Pressure With Mortality and Cardiovascular Outcomes
- PMID: 31386134
- PMCID: PMC6822661
- DOI: 10.1001/jama.2019.9811
Association of Office and Ambulatory Blood Pressure With Mortality and Cardiovascular Outcomes
Abstract
Importance: Blood pressure (BP) is a known risk factor for overall mortality and cardiovascular (CV)-specific fatal and nonfatal outcomes. It is uncertain which BP index is most strongly associated with these outcomes.
Objective: To evaluate the association of BP indexes with death and a composite CV event.
Design, setting, and participants: Longitudinal population-based cohort study of 11 135 adults from Europe, Asia, and South America with baseline observations collected from May 1988 to May 2010 (last follow-ups, August 2006-October 2016).
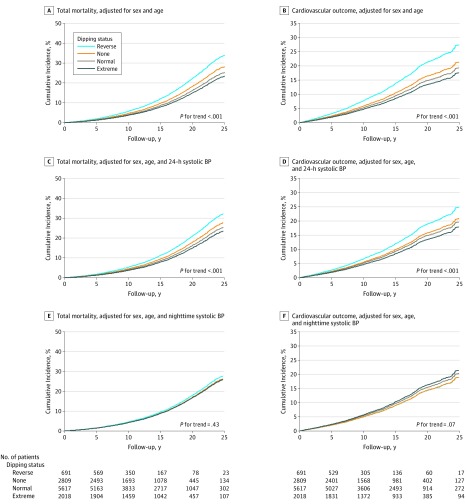
Exposures: Blood pressure measured by an observer or an automated office machine; measured for 24 hours, during the day or the night; and the dipping ratio (nighttime divided by daytime readings).
Main outcomes and measures: Multivariable-adjusted hazard ratios (HRs) expressed the risk of death or a CV event associated with BP increments of 20/10 mm Hg. Cardiovascular events included CV mortality combined with nonfatal coronary events, heart failure, and stroke. Improvement in model performance was assessed by the change in the area under the curve (AUC).
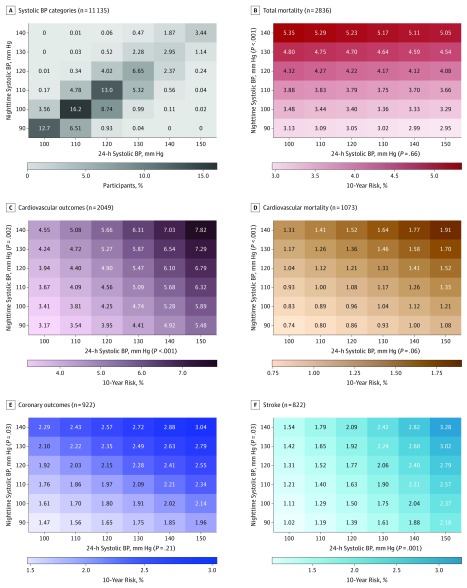
Results: Among 11 135 participants (median age, 54.7 years, 49.3% women), 2836 participants died (18.5 per 1000 person-years) and 2049 (13.4 per 1000 person-years) experienced a CV event over a median of 13.8 years of follow-up. Both end points were significantly associated with all single systolic BP indexes (P < .001). For nighttime systolic BP level, the HR for total mortality was 1.23 (95% CI, 1.17-1.28) and for CV events, 1.36 (95% CI, 1.30-1.43). For the 24-hour systolic BP level, the HR for total mortality was 1.22 (95% CI, 1.16-1.28) and for CV events, 1.45 (95% CI, 1.37-1.54). With adjustment for any of the other systolic BP indexes, the associations of nighttime and 24-hour systolic BP with the primary outcomes remained statistically significant (HRs ranging from 1.17 [95% CI, 1.10-1.25] to 1.87 [95% CI, 1.62-2.16]). Base models that included single systolic BP indexes yielded an AUC of 0.83 for mortality and 0.84 for the CV outcomes. Adding 24-hour or nighttime systolic BP to base models that included other BP indexes resulted in incremental improvements in the AUC of 0.0013 to 0.0027 for mortality and 0.0031 to 0.0075 for the composite CV outcome. Adding any systolic BP index to models already including nighttime or 24-hour systolic BP did not significantly improve model performance. These findings were consistent for diastolic BP.
Conclusions and relevance: In this population-based cohort study, higher 24-hour and nighttime blood pressure measurements were significantly associated with greater risks of death and a composite CV outcome, even after adjusting for other office-based or ambulatory blood pressure measurements. Thus, 24-hour and nighttime blood pressure may be considered optimal measurements for estimating CV risk, although statistically, model improvement compared with other blood pressure indexes was small.
Conflict of interest statement
Figures
Comment in
-
Effective Use of Ambulatory Blood Pressure Monitoring.JAMA. 2019 Aug 6;322(5):420-421. doi: 10.1001/jama.2019.10123. JAMA. 2019. PMID: 31386117 No abstract available.
-
Blood Pressure Indexes Associated With Mortality and Cardiovascular Outcomes.JAMA. 2019 Dec 17;322(23):2342-2343. doi: 10.1001/jama.2019.16836. JAMA. 2019. PMID: 31846010 No abstract available.
References
-
- Leung AA, Nerenberg K, Daskalopoulou SS, et al. ; CHEP Guidelines Task Force . Hypertension Canada’s 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2016;32(5):569-588. doi: 10.1016/j.cjca.2016.02.066 - DOI - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006 - DOI - PubMed
-
- National Institute for Health and Clinical Excellence (NICE) Hypertension in adults: diagnosis and management. http://www.nice.org.uk/guidance/CG127. Published August 2011. Updated November 2016. Accessed June 3, 2019.
-
- Shimamoto K, Ando K, Fujita T, et al. ; Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension . The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2014). Hypertens Res. 2014;37(4):253-390. doi: 10.1038/hr.2014.20 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
