

Dietary patterns and risk of incident chronic kidney disease: the Atherosclerosis Risk in Communities study
- PMID: 31386145
- PMCID: PMC6736122
- DOI: 10.1093/ajcn/nqz146
Dietary patterns and risk of incident chronic kidney disease: the Atherosclerosis Risk in Communities study
Abstract
Background: Adherence to healthy dietary patterns, measured by the Healthy Eating Index (HEI), Alternative Healthy Eating Index (AHEI), and alternate Mediterranean diet (aMed) scores, is associated with a reduced risk of cardiovascular disease. The association between these scores and chronic kidney disease (CKD) is undetermined.
Objective: We aimed to estimate the association between the HEI, AHEI, and aMed scores and risk of incident CKD.
Methods: We conducted a prospective analysis in 12,155 participants aged 45-64 y from the Atherosclerosis Risk in Communities (ARIC) Study. We calculated HEI-2015, AHEI-2010, and aMed scores for each participant and categorized them into quintiles of each dietary score. Incident CKD was defined as an estimated glomerular filtration rate <60 mL/min/1.73 m2 accompanied by ≥25% decline in estimated glomerular filtration rate, a kidney disease-related hospitalization or death, or end-stage renal disease. We used cause-specific hazard models to estimate risk of CKD from the quintile of the dietary score through to 31 December 2017.
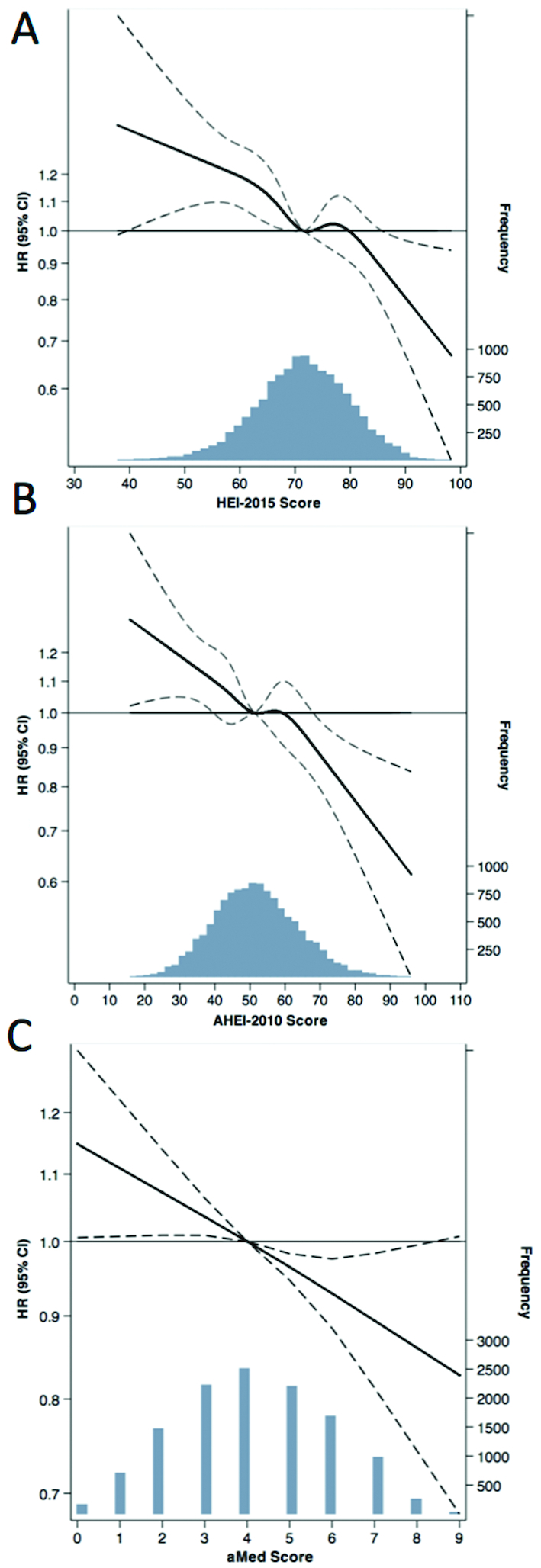
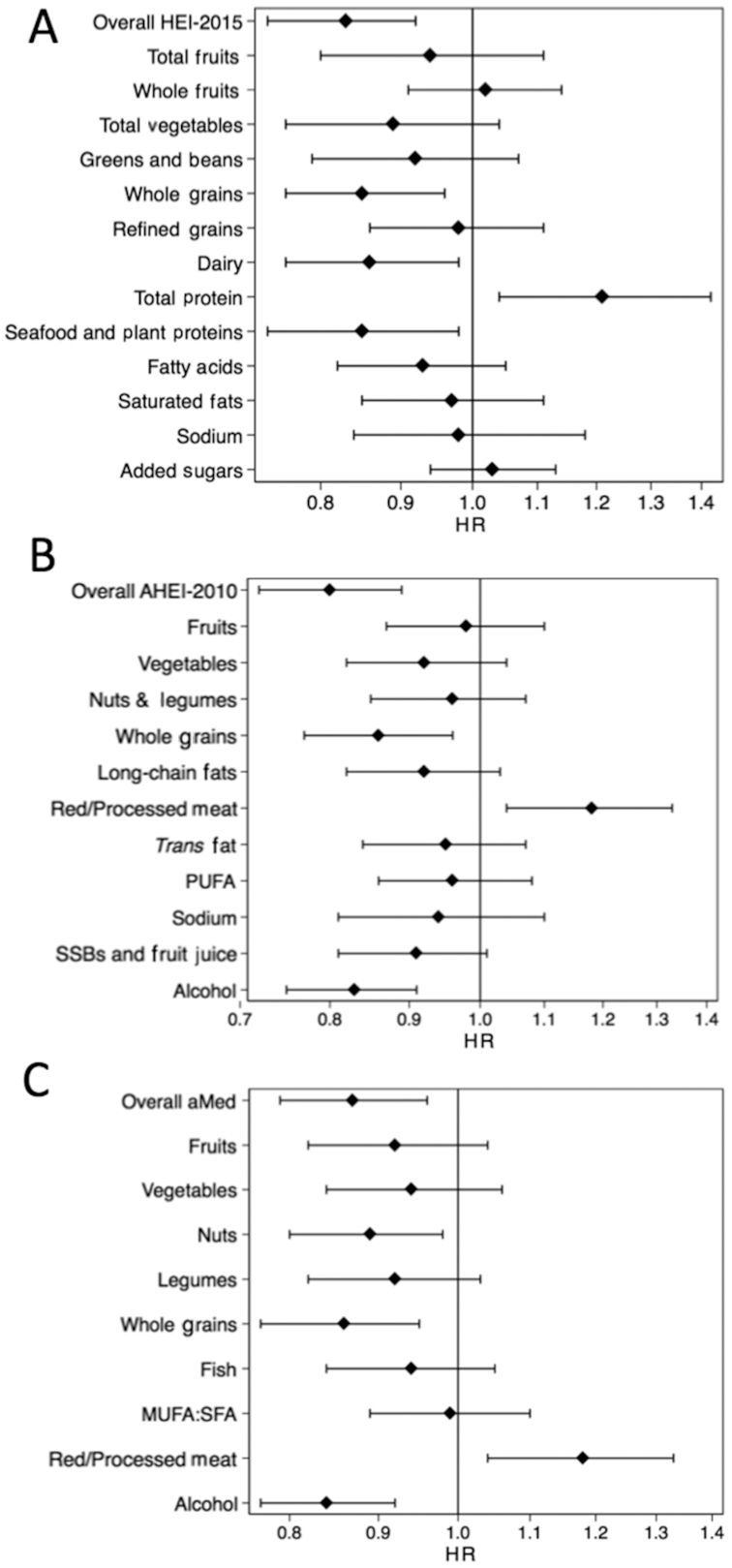
Results: There were 3980 cases of incident CKD over a median follow-up of 24 y. Participants who had higher adherence to the HEI-2015, AHEI-2010, and aMed scores were more likely to be female, have higher educational attainment, higher income level, be nonsmokers, more physically active, and diabetic compared with participants who scored lower. All 3 dietary scores were associated with lower CKD risk (P-trend < 0.001). Participants who were in the highest quintile of HEI-2015 score had a 17% lower risk of CKD (HR: 0.83; 95% CI: 0.74, 0.92) compared with participants in the lowest quintile. Those in quintile 5 of AHEI-2010 and aMed scores, respectively, had a 20% and 13% lower risk of CKD compared with those in quintile 1.
Conclusion: Higher adherence to healthy dietary patterns during middle age was associated with lower risk of CKD.
Keywords: AHEI; ARIC; DASH; HEI; Mediterranean; dietary patterns; dietary scores; kidney disease; renal disease.
Copyright © American Society for Nutrition 2019.
Figures
References
-
- Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi T, Azizi F. Beneficial effects of a Dietary Approaches to Stop Hypertension eating plan on features of the metabolic syndrome. Diabetes Care. 2005;28(12):2823–31. - PubMed
-
- Fung TT, Chiuve SE, McCullough ML, Rexrode KM, Logroscino G, Hu FB. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med. 2008;168(7):713–20. - PubMed
-
- Fung TT, McCullough ML, Newby PK, Manson JE, Meigs JB, Rifai N, Willett WC, Hu FB. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am J Clin Nutr. 2005;82(1):163–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
