

The maxillary sinus: physiology, development and imaging anatomy
- PMID: 31386556
- PMCID: PMC6951102
- DOI: 10.1259/dmfr.20190205
The maxillary sinus: physiology, development and imaging anatomy
Erratum in
-
Correction to The maxillary sinus: physiology, development and imaging anatomy.Dentomaxillofac Radiol. 2019 Dec;48(8):20190205c. doi: 10.1259/dmfr.20190205.c. Epub 2019 Sep 10. Dentomaxillofac Radiol. 2019. PMID: 31502867 Free PMC article. No abstract available.
Abstract
Objectives: The maxillary sinus is of paramount importance for otolaryngologists, rhinologists, oral and maxillofacial surgeons, head and neck and dental and maxillofacial radiologists. A comprehensive review article concerning the physiology, development and imaging anatomy was undertaken.
Methods: Relevant literature pertaining to the physiology of the sinonasal cavity, development of the paranasal sinuses and imaging anatomy of the maxilla and maxillary sinus from 2000 to 2019 was reviewed. Emphasis was placed on literature from the last 5 years.
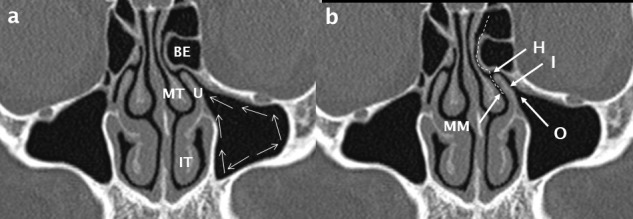
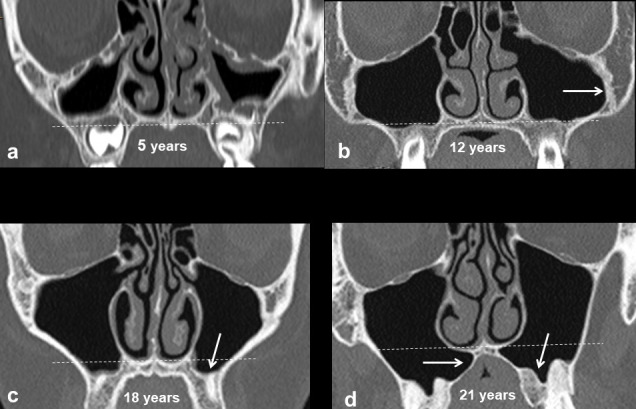
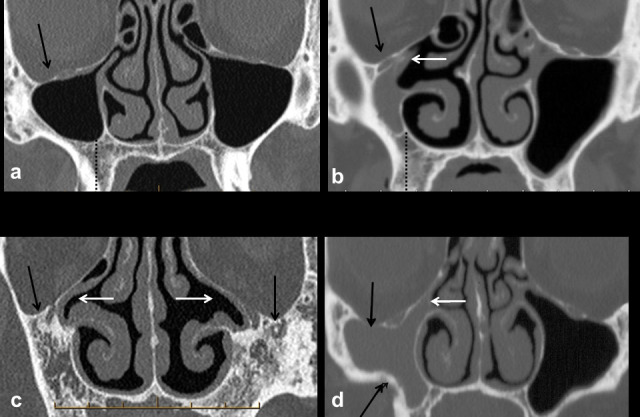
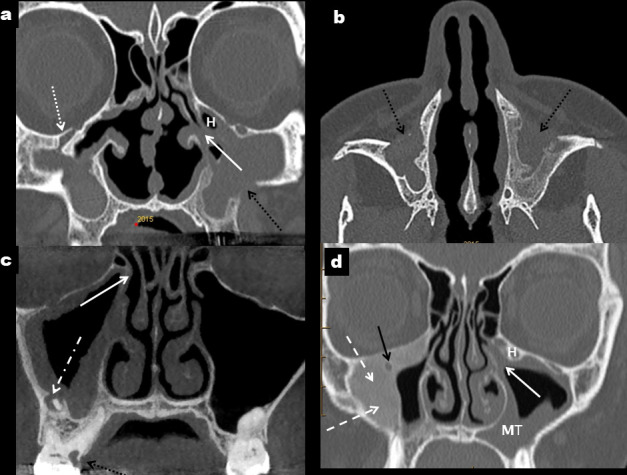
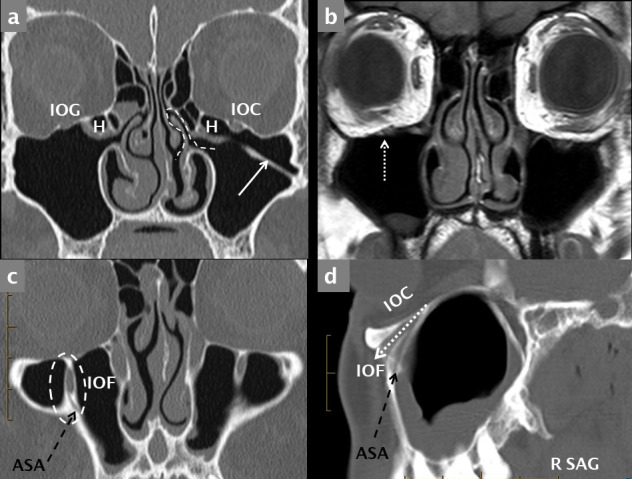
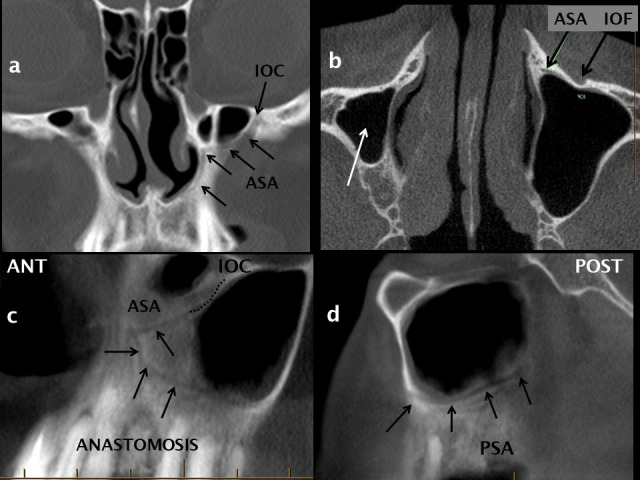
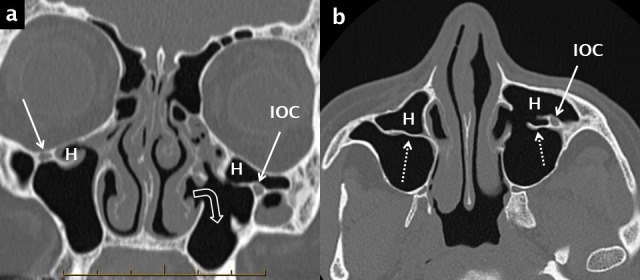
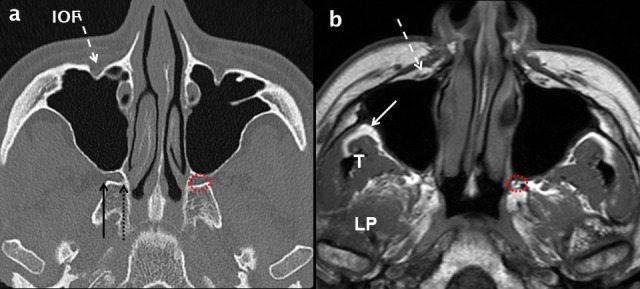
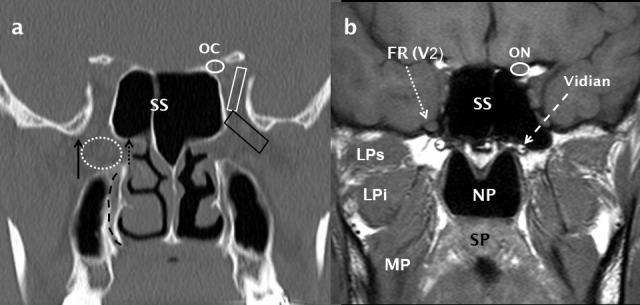
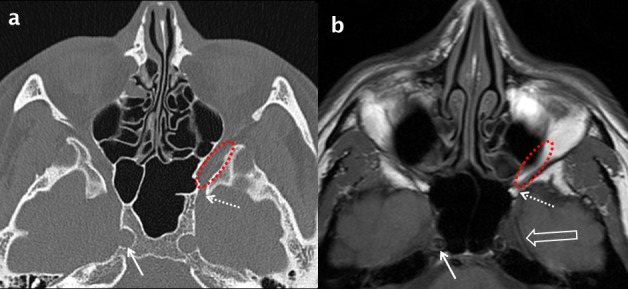
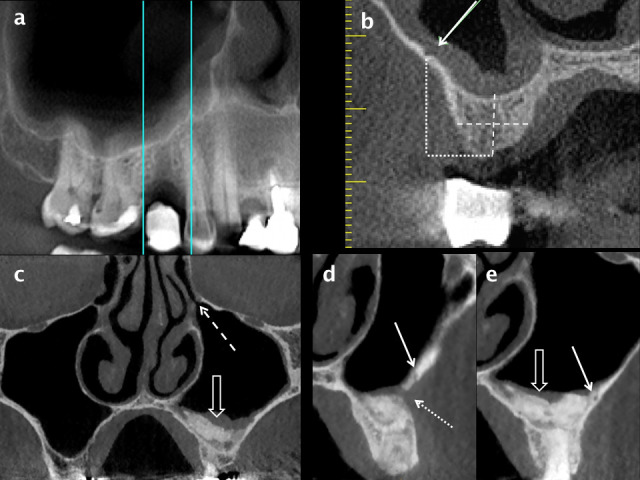
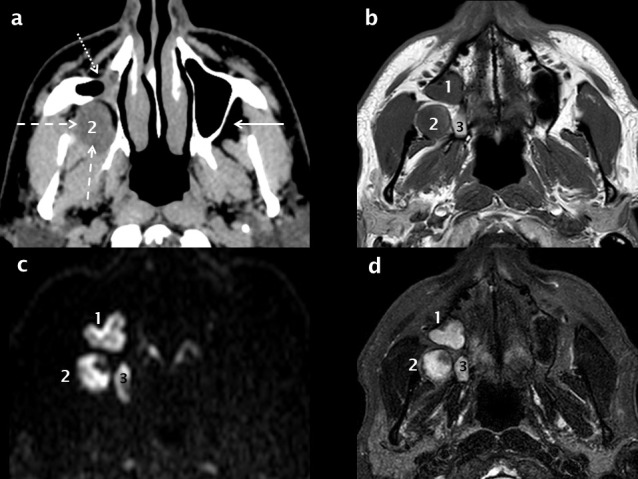
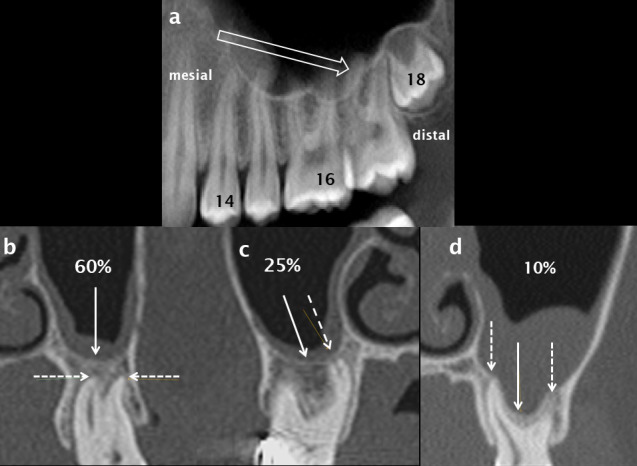
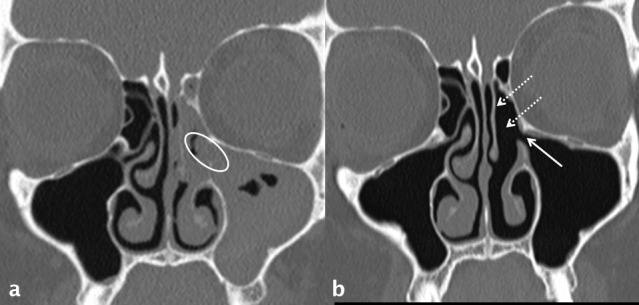
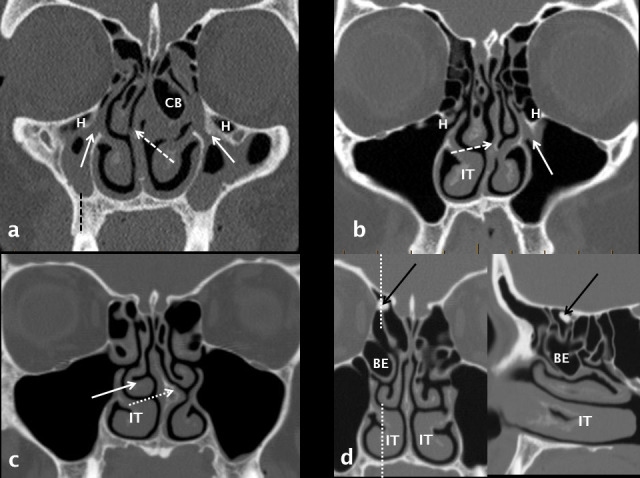
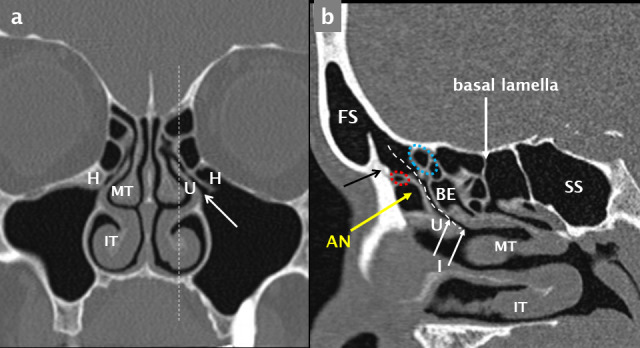
Results: Extensive recent research using imaging has provided new insights into the development of the maxillary sinus, the other paranasal sinuses and the midface. The fundamental physiological concept of mucociliary clearance and its role in sinus health is emphasized. The paranasal sinuses are an integral part of a common mucosal organ formed by the upper and lower airway.An in-depth understanding of the soft-tissue and neurovascular relationships of the maxillary sinus to the deep fascial spaces and branches of the trigeminal nerve and external carotid artery respectively is required to evaluate and report imaging involving the maxillary sinus.Sinusitis of rhinogenic, rather than odontogenic origin, originates from nasal inflammation followed by anterior ethmoid disease and secondary obstruction of the ostiomeatal unit. The role of anatomical variants that predispose to this pattern of disease is discussed in detail with illustrative examples.The maxillary sinus is intimately related to the roots of the posterior maxillary teeth; the high frequency of mucosal disease and sinusitis of odontogenic aetiology is now well recognized. In addition, an understanding of the anatomy of the alveolar process, morphology of the alveolar recess of the maxillary sinus and neurovascular supply are essential both for deliberate surgical intervention of the sinus and complications related to oral surgical procedures.
Conclusions: An understanding of the fundamental principles of the development, physiology, anatomy and relationships of the maxillary sinus as depicted by multi-modality imaging is essential for radiologists reporting imaging involving the paranasal sinuses and midface.
Keywords: Dentition – Anatomy; Diagnostic Imaging; Maxillary Sinus; Physiology.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
