

Procalcitonin and lung ultrasonography point-of-care testing to decide on antibiotic prescription in patients with lower respiratory tract infection in primary care: protocol of a pragmatic cluster randomized trial
- PMID: 31387559
- PMCID: PMC6683414
- DOI: 10.1186/s12890-019-0898-3
Procalcitonin and lung ultrasonography point-of-care testing to decide on antibiotic prescription in patients with lower respiratory tract infection in primary care: protocol of a pragmatic cluster randomized trial
Abstract
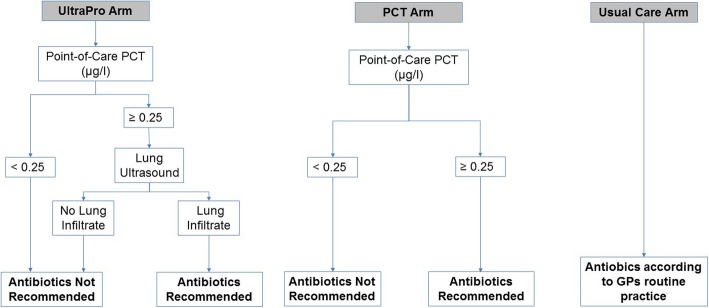
Background: A minority of patients presenting with lower respiratory tract infection (LRTI) to their general practitioner (GP) have community-acquired pneumonia (CAP) and require antibiotic therapy. Identifying them is challenging, because of overlapping symptomatology and low diagnostic performance of chest X-ray. Procalcitonin (PCT) can be safely used to decide on antibiotic prescription in patients with LRTI. Lung ultrasound (LUS) is effective in detecting lung consolidation in pneumonia and might compensate for the lack of specificity of PCT. We hypothesize that combining PCT and LUS, available as point-of care tests (POCT), might reduce antibiotic prescription in LRTIs without impacting patient safety in the primary care setting.
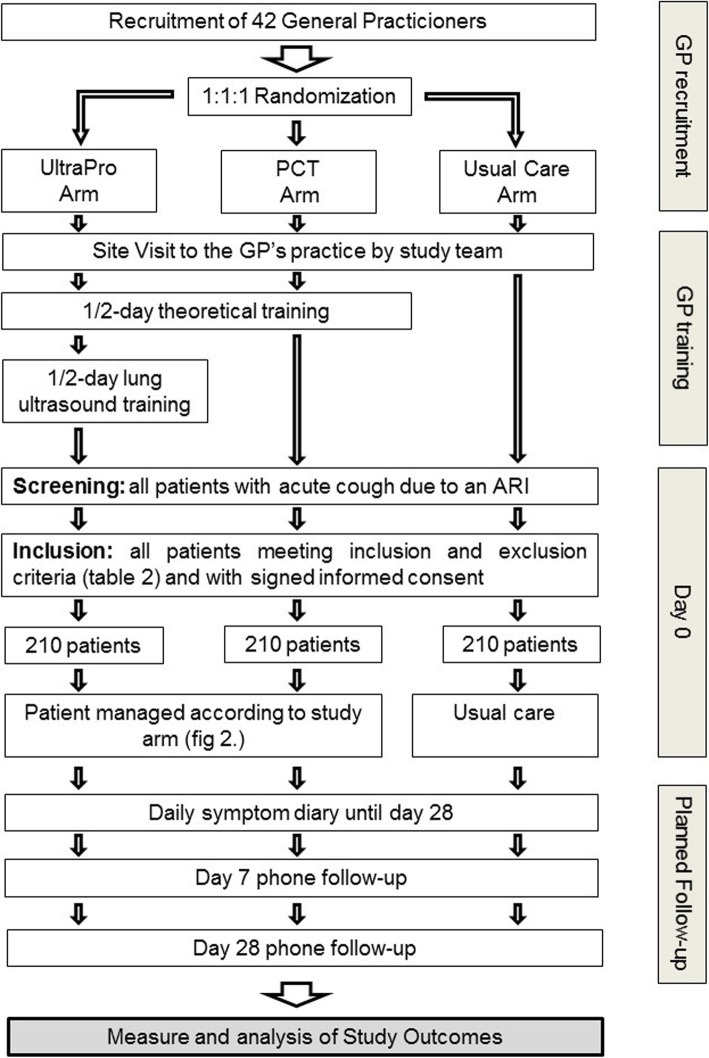
Methods: This is a three-arm pragmatic cluster randomized controlled clinical trial. GPs are randomized either to PCT and LUS-guided antibiotic therapy or to PCT only-guided therapy or to usual care. Consecutive adult patients with an acute cough due to a respiratory infection will be screened and included if they present a clinical pneumonia as defined by European guidelines. Exclusion criteria are previous antibiotics for the current episode, working diagnosis of sinusitis, severe underlying lung disease, severe immunosuppression, hospital admission, pregnancy, inability to provide informed consent and unavailability of the GP. Patients will fill in a 28 day-symptom diary and will be contacted by phone on days 7 and 28. The primary outcome is the proportion of patients prescribed any antibiotic up to day 28. Secondary outcomes include clinical failure by day 7 (death, admission to hospital, absence of amelioration or worsening of relevant symptoms) and by day 28, duration of restricted daily activities, episode duration as defined by symptom score, number of medical visits, number of days with side effects due to antibiotics and a composite outcome combining death, admission to hospital and complications due to LRTI by day 28. An evaluation of the cost-effectiveness and of processes in the clinic using a mixed qualitative and quantitative approach will also be conducted.
Discussion: Our intervention targets only patients with clinically suspected CAP who have a higher pretest probability of definite pneumonia. The intervention will not substitute clinical assessment but completes it by introducing new easy-to-perform tests.
Trial registration: The study was registered on the 19th of June 2017 on the clinicaltrials.gov registry using reference number; NCT03191071 .
Keywords: Antibiotic prescription; General practice; Lower respiratory tract infections; Lung ultrasound; Point of care testing; Procalcitonin.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hurlimann D, Limacher A, Schabel M, Zanetti G, Berger C, Muhlemann K, Kronenberg A, Swiss Sentinel Working G. Improvement of antibiotic prescription in outpatient care: a cluster-randomized intervention study using a sentinel surveillance network of physicians. J Antimicrob Chemother. 2015;70(2):602–608. doi: 10.1093/jac/dku394. - DOI - PubMed
-
- Health FOoP . Joint report 2016. Usage of antibiotics and occurrence of antibiotic resistance in Bacteria from humans and animals in Switzerland. 2016.
-
- Schappert SM, Burt CW. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001-02. Vital Health Stat. 2006;13(159):1–66. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
