

How can CO2-derived indices guide resuscitation in critically ill patients?
- PMID: 31388457
- PMCID: PMC6642918
- DOI: 10.21037/jtd.2019.07.10
How can CO2-derived indices guide resuscitation in critically ill patients?
Abstract
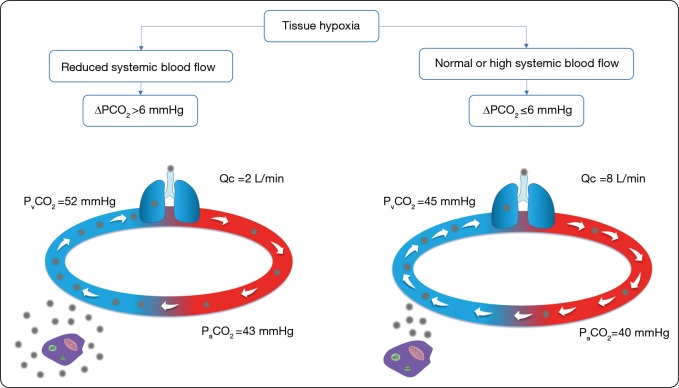
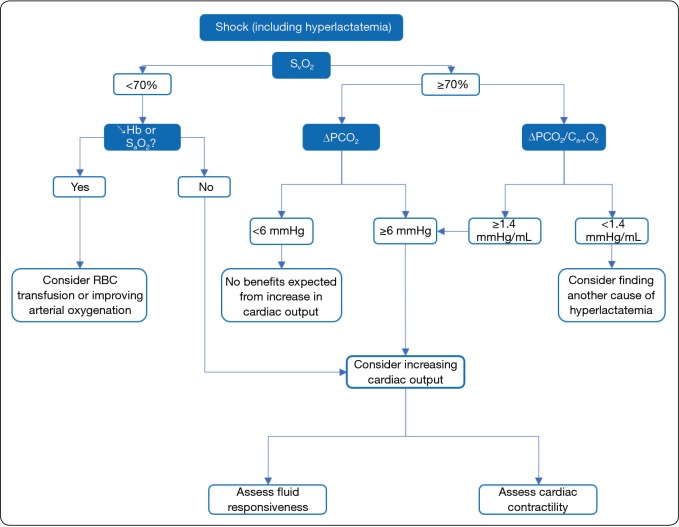
Assessing the adequacy of oxygen delivery with oxygen requirements is one of the key-goal of haemodynamic resuscitation. Clinical examination, lactate and central or mixed venous oxygen saturation (SvO2 and ScvO2, respectively) all have their limitations. Many of them may be overcome by the use of the carbon dioxide (CO2)-derived variables. The venoarterial difference in CO2 tension ("ΔPCO2" or "PCO2 gap") is not an indicator of anaerobic metabolism since it is influenced by the oxygen consumption. By contrast, it reliably indicates whether blood flow is sufficient to carry CO2 from the peripheral tissue to the lungs in view of its clearance: it, thus, reflects the adequacy of cardiac output with the metabolic condition. The ratio of the PCO2 gap with the arteriovenous difference of oxygen content (PCO2 gap/Ca-vO2) might be a marker of anaerobiosis. Conversely to SvO2 and ScvO2, it remains interpretable if the oxygen extraction is impaired as it is in case of sepsis. Compared to lactate, it has the main advantage to change without delay and to provide a real-time monitoring of tissue hypoxia.
Keywords: PCO2 gap; cardiac output; lactate; respiratory quotient; tissue hypoxia.
Conflict of interest statement
Conflicts of Interest: JL Teboul and X Monnet are members of the Medical Advisory Board of Pulsion Medical Systems, Getinge. F Gavelli has no conflicts of interest to declare.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous