

ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection
- PMID: 31388606
- PMCID: PMC6669323
- DOI: 10.1016/j.vgie.2019.03.010
ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection
Abstract
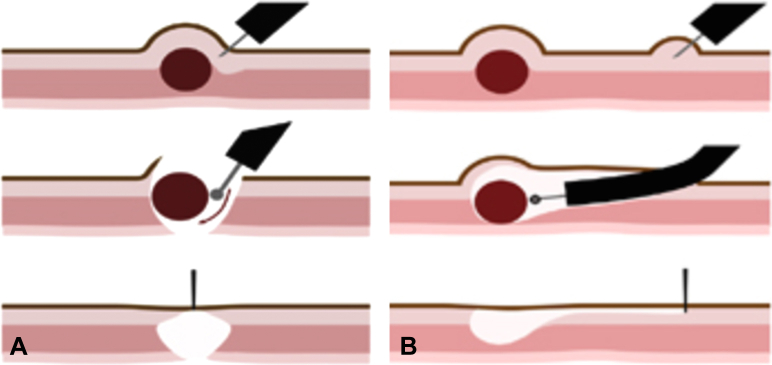
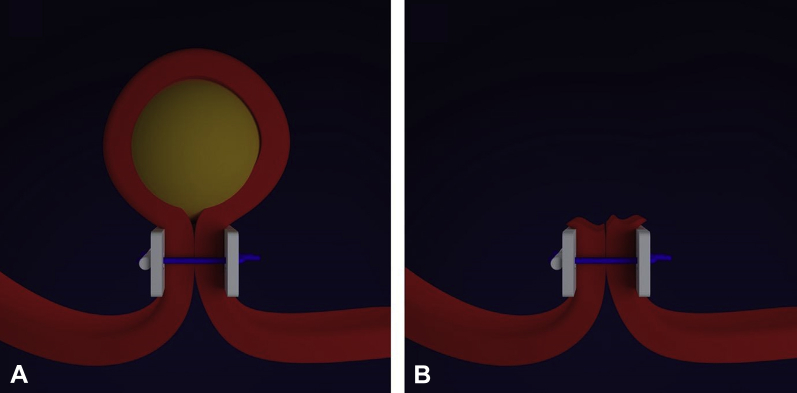
With the development of reliable endoscopic closure techniques and tools, endoscopic full-thickness resection (EFTR) is emerging as a therapeutic option for the treatment of subepithelial tumors and epithelial neoplasia with significant fibrosis. EFTR may be categorized as "exposed" and "nonexposed." In exposed EFTR, the full-thickness resection is undertaken with a tunneled or nontunneled technique, with subsequent closure of the defect. In nonexposed EFTR, a secure serosa-to-serosa apposition is achieved before full-thickness resection of the isolated lesion. This document reviews current techniques and devices used for EFTR and reviews clinical applications and outcomes.
Keywords: EFTR, endoscopic full-thickness resection; ESD, endoscopic submucosal dissection; GIST, GI stromal tumor; NOTES, natural orifice transluminal endoscopic surgery; OTSC, over-the-scope clip; POEM, per-oral endoscopic myotomy; PTFE, polytetrafluoroethylene; SET, subepithelial tumor; STER, submucosal tunnel endoscopic resection; TTS, through-the-scope.
Figures


References
-
- Kashab M.A., Pasricha P.J. Conquering the third space: challenges and opportunities for diagnostic and therapeutic endoscopy. Gastrointest Endosc. 2013;77:146–148. - PubMed
-
- Modayil R., Stavropoulos S. A Western prospective on new NOTES: from POEM to full thickness resection and beyond. Gastrointest Endosc Clin N Am 26. 2016;26:413–432. - PubMed
-
- ASGE Technology Committee. Pannala R., Abu Dayyeh B.K., Aslanian H.R. Per-oral endoscopic myotomy (with video) Gastrointest Endosc. 2016;83:1051–1060. - PubMed
-
- ASGE Technology Committee. Kantsevoy S.V., Adler D.G., Chand B. Natural orifice translumenal endoscopic surgery. Gastrointest Endosc. 2008;68:617–620. - PubMed
-
- ASGE Technology Committee. Maple J.T., Abu Dayyeh B.K., Chauhan S.S. Endoscopic submucosal dissection. Gastrointest Endosc. 2015;81:1311–1325. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
