

Prognostic significance of inflammatory biomarkers in hepatocellular carcinoma following hepatic resection
- PMID: 31388642
- PMCID: PMC6677099
- DOI: 10.1002/bjs5.50170
Prognostic significance of inflammatory biomarkers in hepatocellular carcinoma following hepatic resection
Abstract
Background: Cancer-related inflammation has been correlated with cancer prognosis. This study evaluated inflammatory biomarkers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR), programmed death ligand (PD-L) 1 expression, and tumour microenvironment in relation to prognosis and clinicopathological features of patients with hepatocellular carcinoma (HCC) undergoing curative hepatic resection.
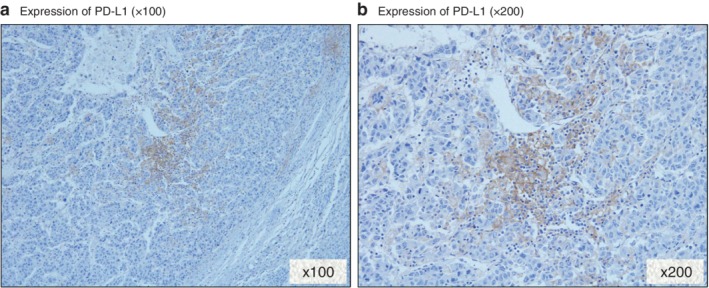
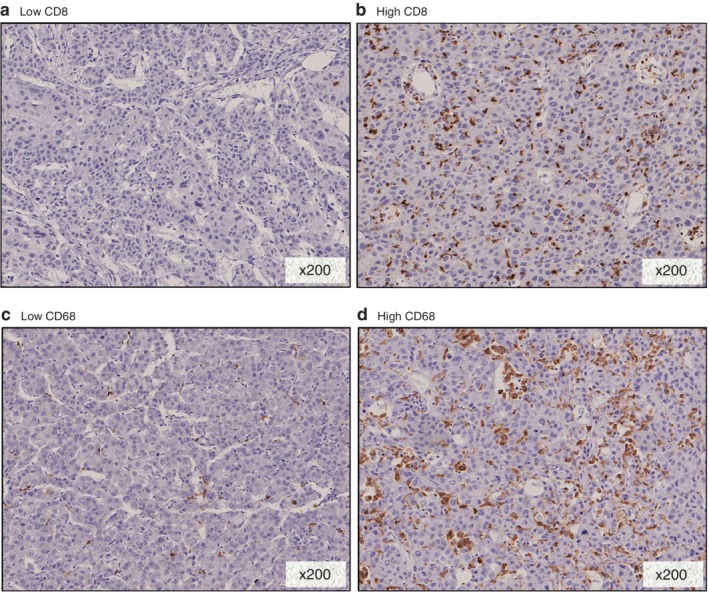
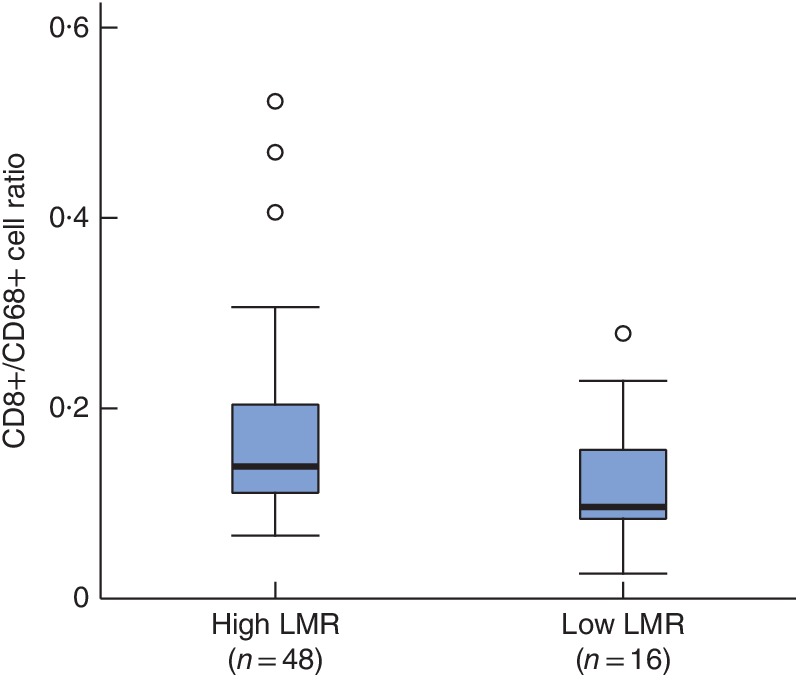
Methods: Patients who had liver resection for HCC in 2000-2011 were analysed. Univariable and multivariable analyses were conducted for overall (OS) and recurrence-free (RFS) survival. Immunohistochemical analyses of PD-L1, CD8 and CD68 expression were performed. HCC cell lines were evaluated for PD-L1 expression. A subgroup analysis was conducted to determine patient features, survival and the tumour microenvironment. Results were validated in a cohort of patients with HCC treated surgically in 2012-2016.
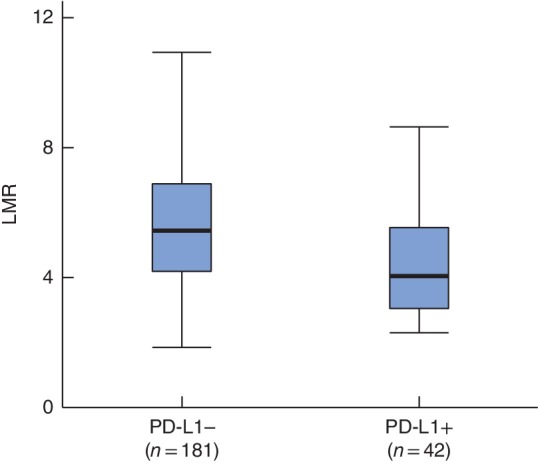
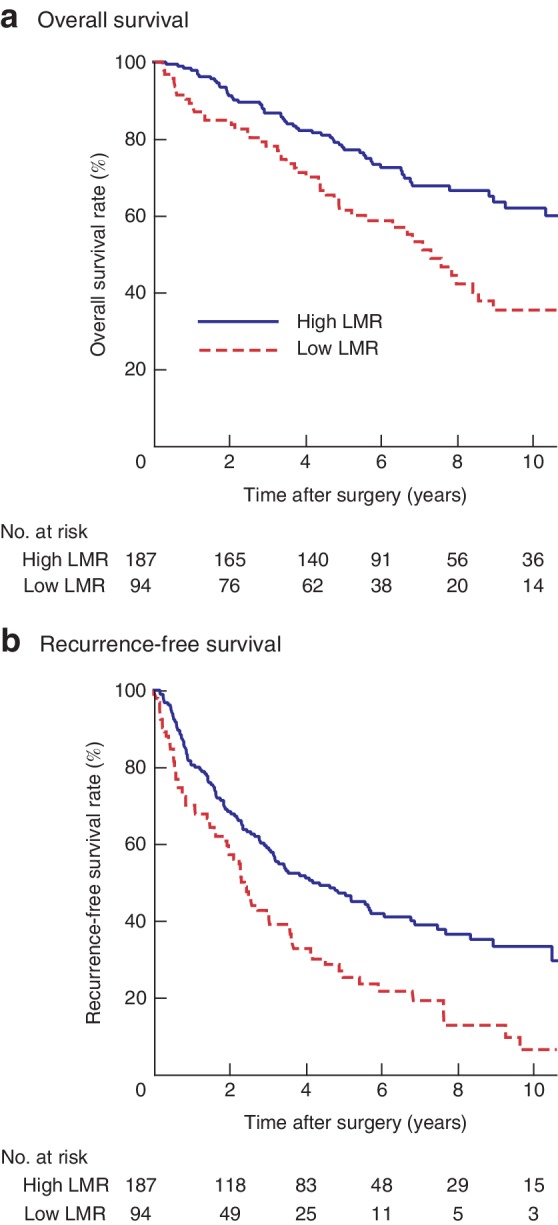
Results: Some 281 patients who underwent hepatic resection for HCC were included. Multivariable analysis showed that low LMR was an independent prognostic factor of OS (hazard ratio (HR) 1·59, 95 per cent c.i. 1·00 to 2·41; P = 0·045) and RFS (HR 1·47, 1·05 to 2·04; P = 0·022) after resection. Low preoperative LMR values were correlated with higher α-fetoprotein values (P < 0·001), larger tumour size (P < 0·001), and high rates of poor differentiation (P = 0·035) and liver cirrhosis (P = 0·008). LMR was significantly lower in PD-L1-positive patients than in those with PD-L1 negativity (P < 0·001). Results were confirmed in the validation cohort. PD-L1 expression was upregulated in HCC cell lines treated with interferon-γ and co-cultured with THP-1 monocyte cells.
Conclusion: LMR is an independent predictor of survival after hepatic resection in patients with HCC. Modulation of the immune checkpoint pathway in the tumour microenvironment is associated with a low LMR.
Figures
References
-
- Bosetti C, Turati F, La Vecchia C. Hepatocellular carcinoma epidemiology. Best Pract Res Clin Gastroenterol 2014; 28: 753–770. - PubMed
-
- Itoh S, Morita K, Ueda S, Sugimachi K, Yamashita Y, Gion T et al Long‐term results of hepatic resection combined with intraoperative local ablation therapy for patients with multinodular hepatocellular carcinomas. Ann Surg Oncol 2009; 16: 3299–3307. - PubMed
-
- Itoh S, Shirabe K, Taketomi A, Morita K, Harimoto N, Tsujita E et al Zero mortality in more than 300 hepatic resections: validity of preoperative volumetric analysis. Surg Today 2012; 42: 435–440. - PubMed
-
- Elinav E, Nowarski R, Thaiss CA, Hu B, Jin C, Flavell RA. Inflammation‐induced cancer: crosstalk between tumours, immune cells and microorganisms. Nat Rev Cancer 2013; 13: 759–771. - PubMed
-
- Yoshizumi T, Ikegami T, Yoshiya S, Motomura T, Mano Y, Muto J et al Impact of tumor size, number of tumors and neutrophil‐to‐lymphocyte ratio in liver transplantation for recurrent hepatocellular carcinoma. Hepatol Res 2013; 43: 709–716. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
