

The effect of an mHealth clinical decision-making support system on neonatal mortality in a low resource setting: A cluster-randomized controlled trial
- PMID: 31388661
- PMCID: PMC6677648
- DOI: 10.1016/j.eclinm.2019.05.010
The effect of an mHealth clinical decision-making support system on neonatal mortality in a low resource setting: A cluster-randomized controlled trial
Abstract
Background: MHealth interventions promise to bridge gaps in clinical care but documentation of their effectiveness is limited. We evaluated the utilization and effect of an mhealth clinical decision-making support intervention that aimed to improve neonatal mortality in Ghana by providing access to emergency neonatal protocols for frontline health workers.
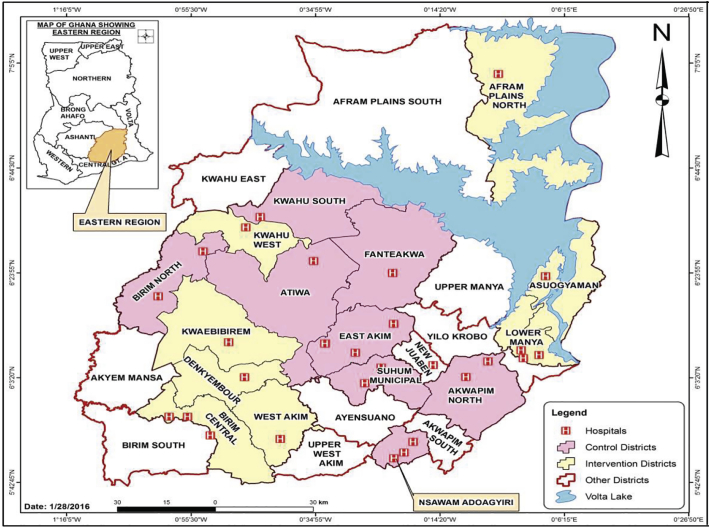
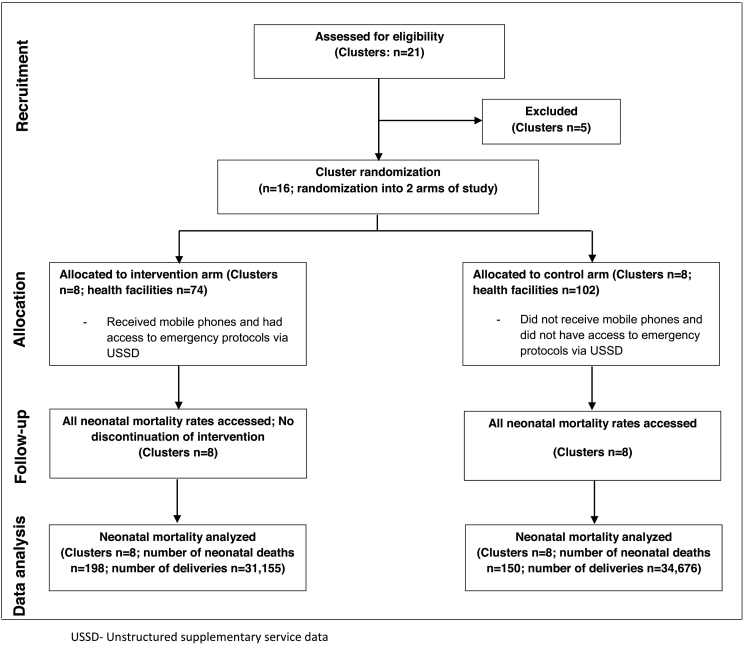
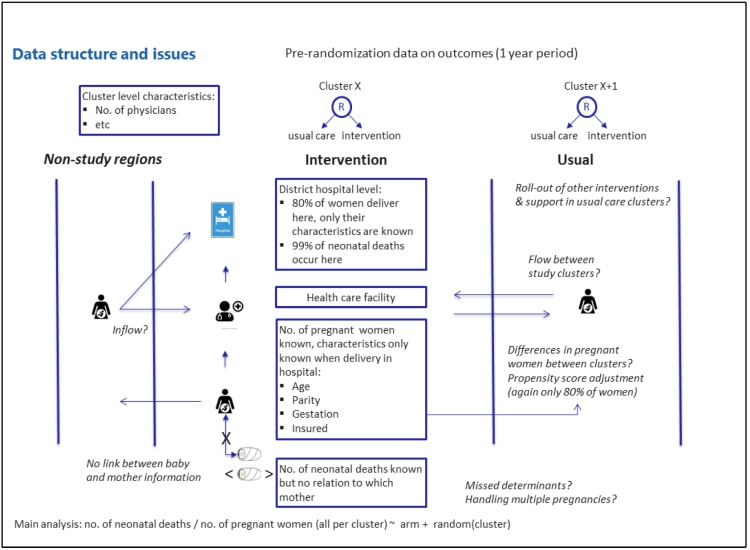
Methods: In the Eastern Region of Ghana, sixteen districts were randomized into two study arms (8 intervention and 8 control clusters) in a cluster-randomized controlled trial. Institutional neonatal mortality data were extracted from the District Health Information System-2 during an 18-month intervention period. We performed an intention-to-treat analysis and estimated the effect of the intervention on institutional neonatal mortality (primary outcome measure) using grouped binomial logistic regression with a random intercept per cluster. This trial is registered at ClinicalTrials.gov (NCT02468310 ) and Pan African Clinical Trials Registry (PACTR20151200109073).
Findings: There were 65,831 institutional deliveries and 348 institutional neonatal deaths during the study period. Overall, 47 ∙ 3% of deliveries and 56 ∙ 9% of neonatal deaths occurred in the intervention arm. During the intervention period, neonatal deaths increased from 4 ∙ 5 to 6 ∙ 4 deaths and, from 3 ∙ 9 to 4 ∙ 3 deaths per 1000 deliveries in the intervention arm and control arm respectively. The odds of neonatal death was 2⋅09 (95% CI (1 ∙ 00;4 ∙ 38); p = 0 ∙ 051) times higher in the intervention arm compared to the control arm (adjusted odds ratio). The correlation between the number of protocol requests and the number of deliveries per intervention cluster was 0 ∙ 71 (p = 0 ∙ 05).
Interpretation: The higher risk of institutional neonatal death observed in intervention clusters may be due to problems with birth and death registration, unmeasured and unadjusted confounding, and unintended use of the intervention. The findings underpin the need for careful and rigorous evaluation of mHealth intervention implementation and effects.
Funding: Netherlands Foundation for Scientific Research - WOTRO, Science for Global Development; Utrecht University.
Keywords: Ghana; Low and middle income countries; Neonatal mortality; mHealth.
Conflict of interest statement
We declare no competing interests.
Figures

References
-
- Organization WH Trends in maternal mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations population division. Geneva, Switzerland. 2015. http://apps.who.int/iris/bitstream/10665/194254/1/9789241565141_eng.pdf?...
-
- Lawn J.E., Cousens S., Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet. 2005;365:891–900. - PubMed
-
- Liu L., Johnson H.L., Cousens S. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–2161. - PubMed
-
- Say L., Chou D., Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Heal. 2014;2:e323–e333. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
