

doi: 10.1007/s00261-019-02170-5.
Rectal cancer lexicon: consensus statement from the society of abdominal radiology rectal & anal cancer disease-focused panel
Affiliations
- PMID: 31388697
- PMCID: PMC6824987
- DOI: 10.1007/s00261-019-02170-5
Item in Clipboard
Rectal cancer lexicon: consensus statement from the society of abdominal radiology rectal & anal cancer disease-focused panel
Abdom Radiol (NY).
2019 Nov.
Abstract
Standardized terminology is critical to providing consistent reports to referring clinicians. This lexicon aims to provide a reference for terminology frequently used in rectal cancer and reflects the consensus of the Society of Abdominal Radiology Disease Focused Panel in Rectal cancer. This lexicon divided the terms into the following categories: primary tumor staging, nodal staging, treatment response, anal canal anatomy, general anatomy, and treatments.
Keywords: Lexicon; MRI; Rectal cancer; Society of Abdominal Radiology Rectal & Anal Cancer Disease-Focused Panel; Staging.
Conflict of interest statement
Figures
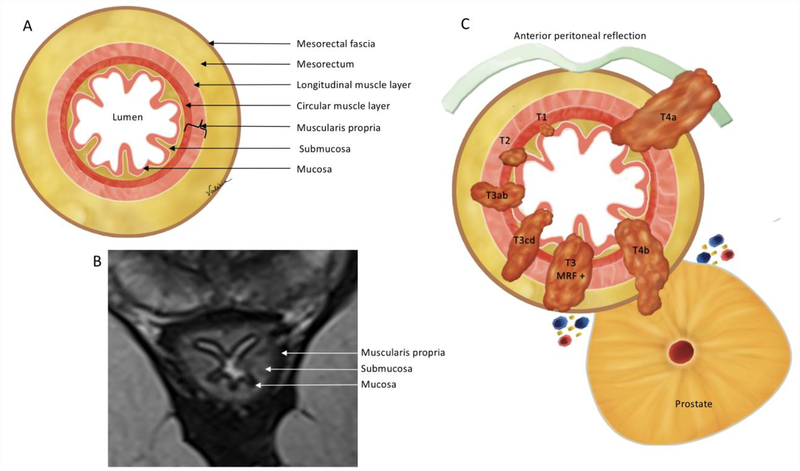
Oblique axial view anatomy. (A) Illustration and (B) high-resolution axial oblique T2WI demonstrate the mesorectal fascia, mesorectum and rectal wall layers. On MRI (B) 3 layers are mostly visible: mucosa, as the innermost thin hypointense layer, submucosa, as a middle hyperintense layer and muscularis propria, as the outer hypointense layer. (C) Illustration demonstrating the T-category. T1 - tumor up to submucosa; T2 - tumor up to muscularis propria; T3 - tumor beyond muscularis propria (T3a < 1 mm, T3b: 1–5 mm, T3c: 5–15 mm, and T4d > 15 mm); T4 - tumor infiltrates the peritoneal reflection (T4a) or other pelvic organs and structures (T4b).
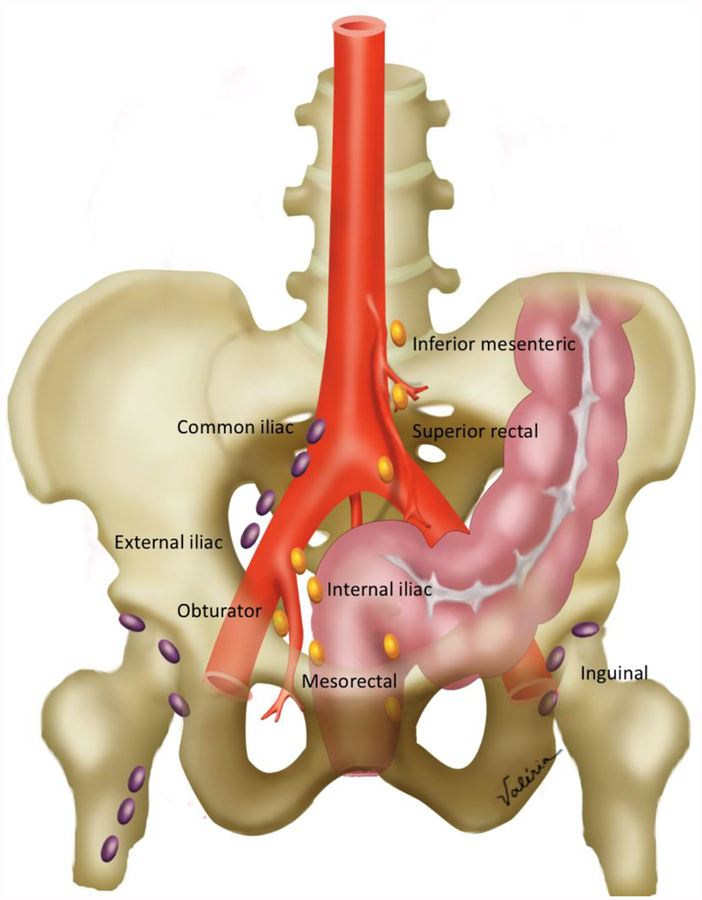
Pelvic nodal anatomy. Locoregional nodes (colored in gold) include the inferior mesenteric, superior rectal, internal iliac, obturator and mesorectal nodes. Non-locoregional nodes (colored in purple) include common iliac, external iliac and inguinal nodes. Obturator nodes are lateral to the internal iliac artery, while internal iliac nodes are medial.
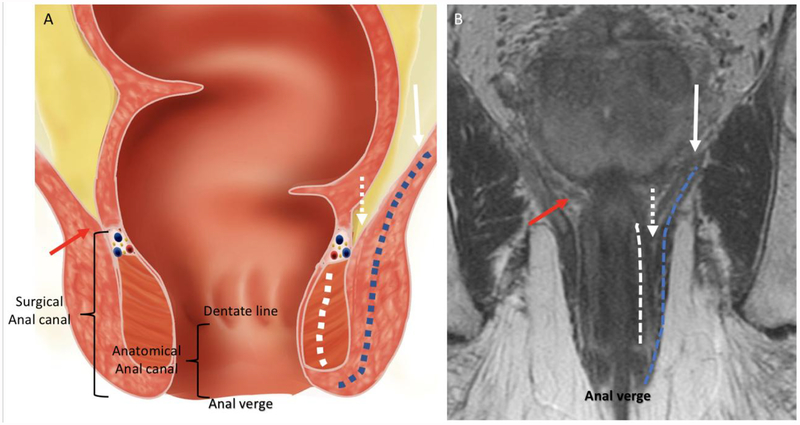
Coronal anatomy of the anal canal. (A) Illustration and (B) coronal T2WI showing the levator ani (white arrow), internal sphincter (dashed white line), external sphincter complex (dashed blue line), intersphincteric plane (dashed white arrows), anorectal junction (red arrows), anal verge, dentate line, anatomical anal canal and surgical anal canal.
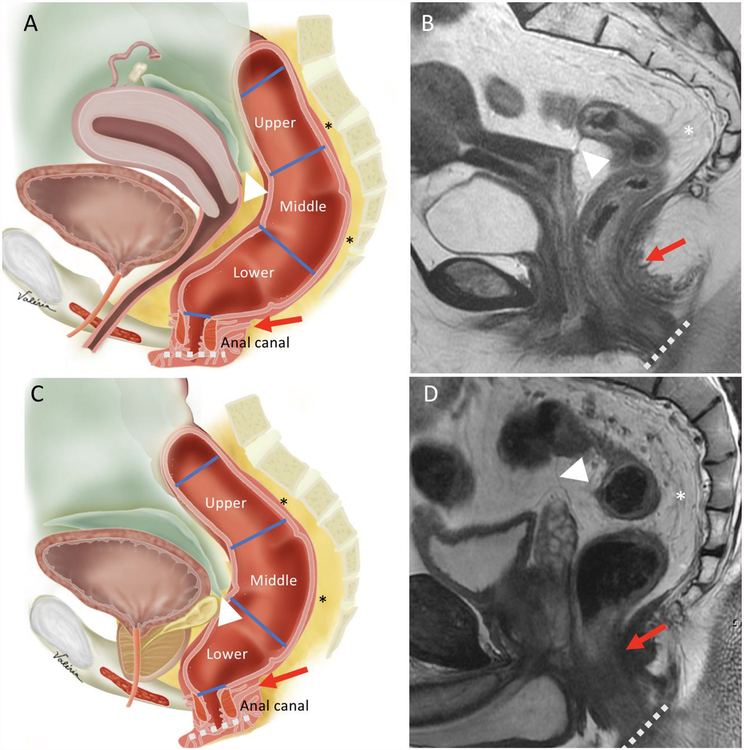
Sagittal view anatomy. Illustrations and sagittal T2WI sequences in female (A-B) and male (C-D) demonstrate the upper, middle and lower rectum, mesorectum (asterisks), anal canal, anterior peritoneal reflection (white arrowheads), anorectal junction (red arrows) and anal verge (dashed lines).
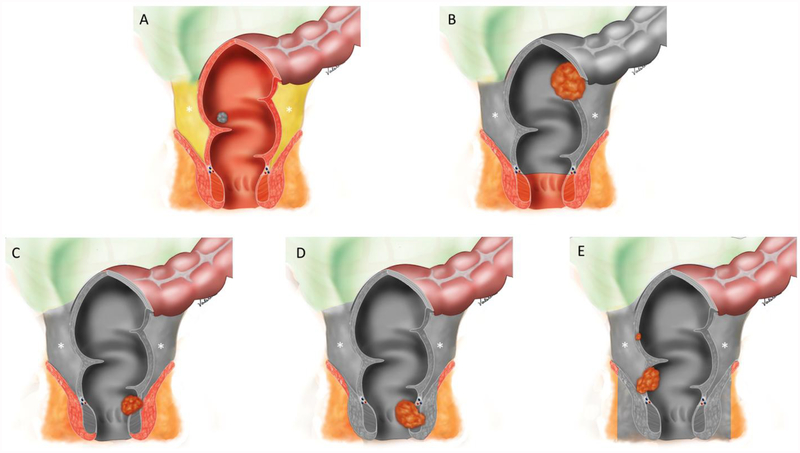
Illustrations demonstrating surgical techniques for rectal cancer: (A) Transanal excision (TAE) / transanal endoscopic microsurgery (TEMS); (B) Low anterior resection (LAR); (C) Intersphincteric abdominoperineal resection; (D) Abdominoperineal resection (APR), and (E) Extralevator abdominoperineal excision (ELAPE). Gray coverage demonstrate the structures that are resected. Note that B-E include total mesorectal excision (TME) with an en bloc resection of the mesorectum (asterisks) through a dissection along the mesorectal fascia.
References
-
- Weiser MR. AJCC 8th Edition: Colorectal Cancer. Annals of surgical oncology. 2018;25:1454–1455. - PubMed
-
- Al-Sukhni E, Milot L, Fruitman M, et al. Diagnostic accuracy of MRI for assessment of T category, lymph node metastases, and circumferential resection margin involvement in patients with rectal cancer: a systematic review and meta-analysis. Annals of surgical oncology. Springer-Verlag. 2012;19:2212–2223. - PubMed
-
- Horvat N, Petkovska I, Gollub MJ. MR Imaging of Rectal Cancer. Radiol Clin North Am. 2018;56:751–774. - PubMed
-
- Beets-Tan RGH, Lambregts DMJ, Maas M, et al. Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting Eur Radiol. Springer Berlin Heidelberg; 2013. pp. 2522–2531. - PubMed
-
- MERCURY Study Group. Extramural depth of tumor invasion at thin-section MR in patients with rectal cancer: results of the MERCURY study. Radiology. 2007;243:132–139. - PubMed
