

Aging effects on pelvic floor support: a pilot study comparing young versus older nulliparous women
- PMID: 31388719
- PMCID: PMC7720445
- DOI: 10.1007/s00192-019-04063-z
Aging effects on pelvic floor support: a pilot study comparing young versus older nulliparous women
Abstract
Introduction and hypothesis: We sought to determine age-related changes to the pelvic floor in the absence of childbirth effects.
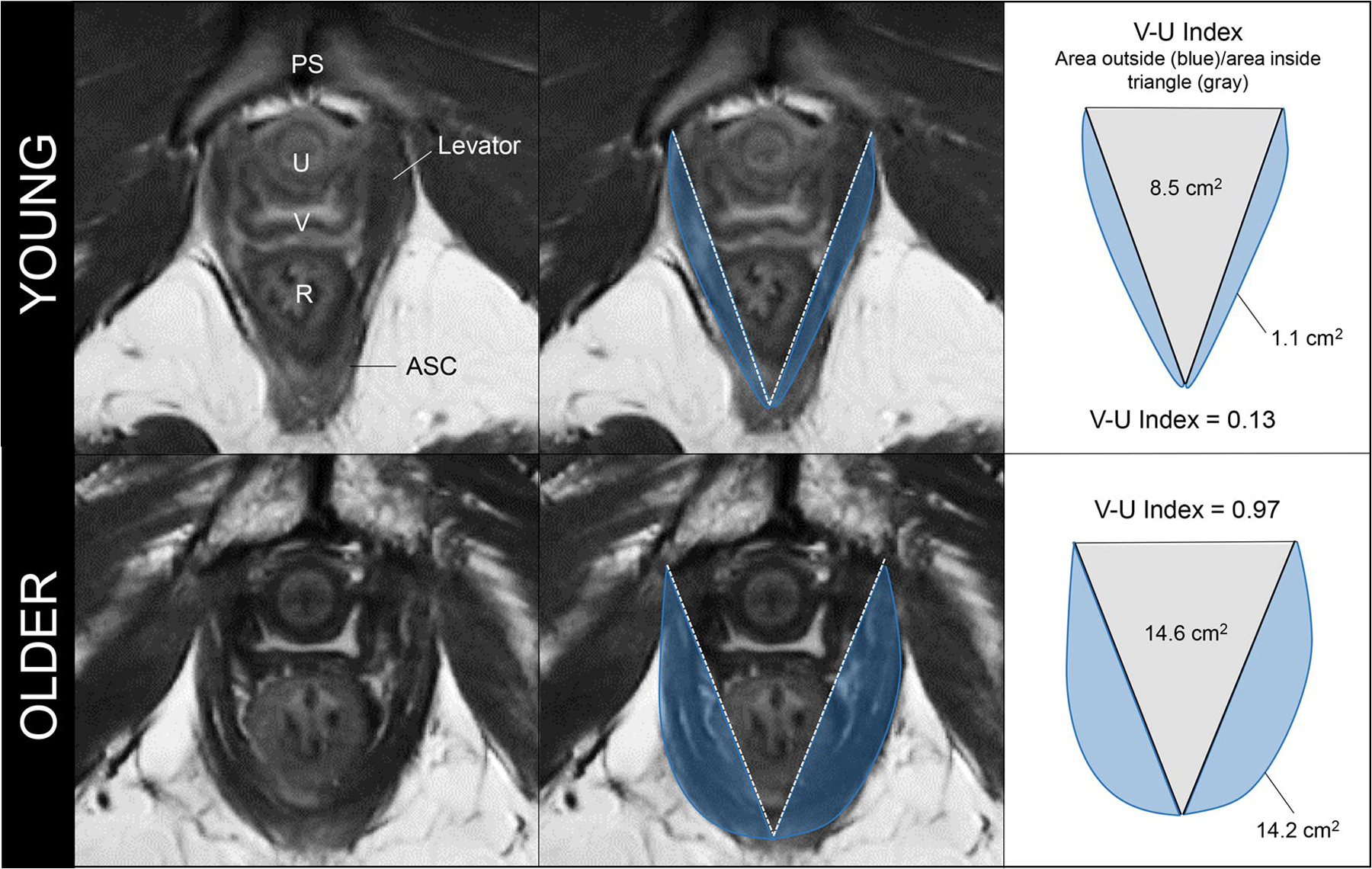
Methods: A case-control study was conducted from June 2017 to August 2018 comparing two groups of nulliparous women: <40 years old and ≥ 70 years old. Clinical evaluation included POP-Q, instrumented speculum testing, and handgrip strength. Dynamic 3D-stress MRI was performed on all women to obtain genital and levator hiatus (LH) lengths, LH area, and levator bowl volume. LH shape was quantified using a novel measure called the "V-U index." Pubovisceral muscle (PVM) cross-sectional area (CSA) was also measured. Bivariate comparisons between the two groups were made for all variables. Effect sizes were calculated for MRI measurements.
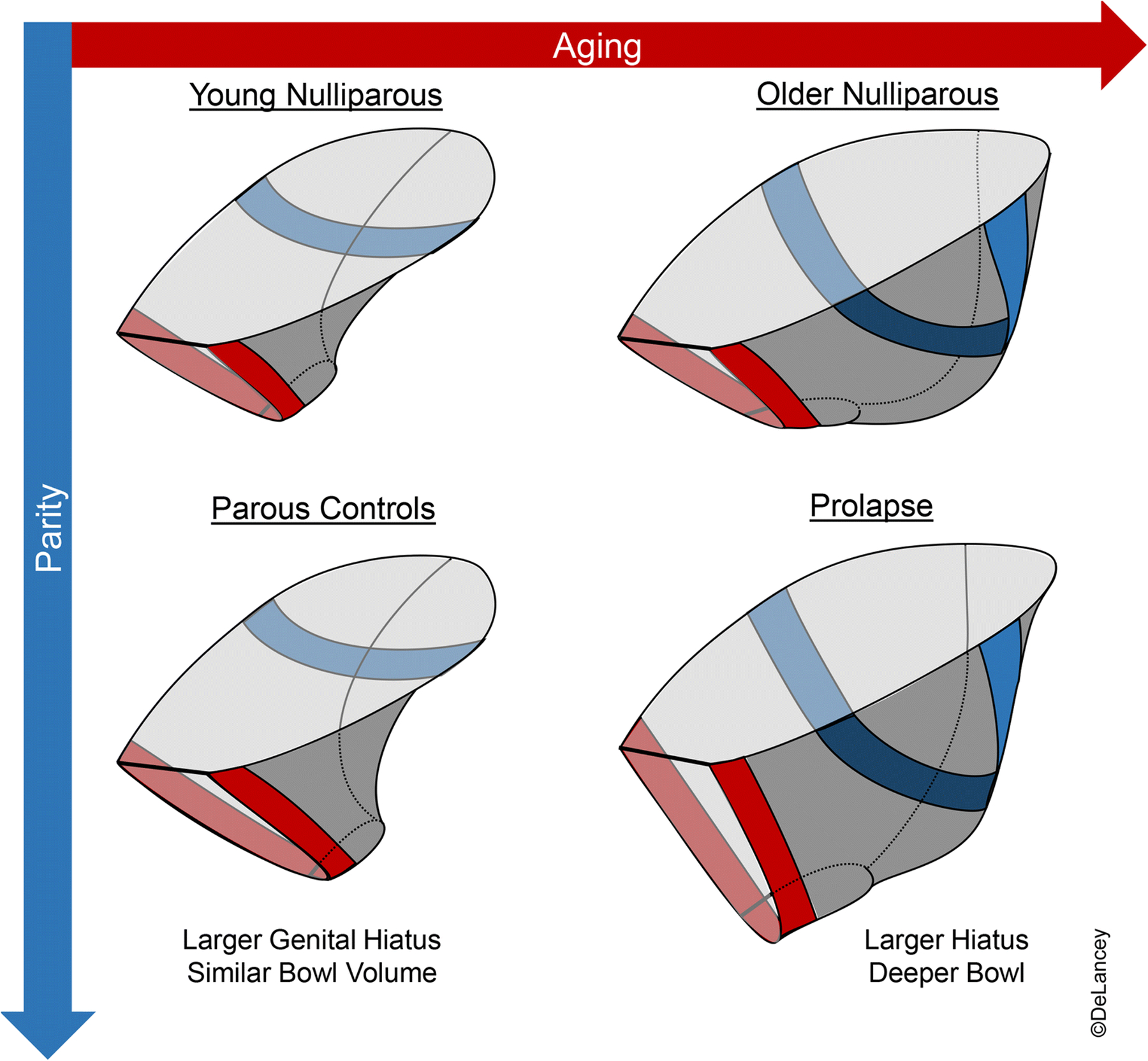
Results: Twelve young and 9 older nulliparous women were included. Levator bowl volume at rest was 83% larger in older women (108.0 ± 34.5 cm3 vs 59.2 ± 19.3 cm3, p = 0.001, d = 1.82). MRI genital hiatus at rest was larger among the older group (2.7 ± 0.6 cm vs 3.5 ± 0.6 cm, p = 0.007, d = 1.34). V-U index, a measure of LH shape where 0 = "V" and 1 = "U," differed between groups indicating a more "U"-like shape among older women (0.71 ± 0.23 vs 0.35 ± 0.18, p = 0.001, d = 1.72). Handgrip strength was lower in the older vs young group (23.2 ± 5.2 N vs 33.4 ± 5.2 N, p < 0.0001); however, the Kegel augmentation force and PVM CSA were similar (3.2 ± 1.1 N vs 3.3 ± 2.2 N, p = 0.89, and 0.8 ± 0.3 cm2 vs 0.7 ± 0.2 cm2, p = 0.23 respectively).
Conclusions: Levator bowl volume at rest was over 80% larger among older women, reflecting a generalized posterior distension with age.
Keywords: Aging; Genital hiatus; Levator area; Levator bowl volume; MRI; Pelvic organ support.
Conflict of interest statement
Figures



References
-
- Mant J, Painter R, Vessey M (1997) Epidemiology of genital prolapse: observations from the Oxford Family Planning Association Study. Br J Obstet Gynaecol 104(5):579–585 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
