

Comparing the McGrath Mac Video Laryngoscope and Direct Laryngoscopy for Prehospital Emergency Intubation in Air Rescue Patients: A Multicenter, Randomized, Controlled Trial
- PMID: 31389835
- PMCID: PMC6791500
- DOI: 10.1097/CCM.0000000000003918
Comparing the McGrath Mac Video Laryngoscope and Direct Laryngoscopy for Prehospital Emergency Intubation in Air Rescue Patients: A Multicenter, Randomized, Controlled Trial
Abstract
Objectives: Tracheal intubation in prehospital emergency care is challenging. The McGrath Mac Video Laryngoscope (Medtronic, Minneapolis, MN) has been proven to be a reliable alternative for in-hospital airway management. This trial compared the McGrath Mac Video Laryngoscope and direct laryngoscopy for the prehospital setting.
Design: Multicenter, prospective, randomized, controlled equivalence trial.
Setting: Oesterreichischer Automobil- und Touring Club (OEAMTC) Helicopter Emergency Medical Service in Austria, 18-month study period.
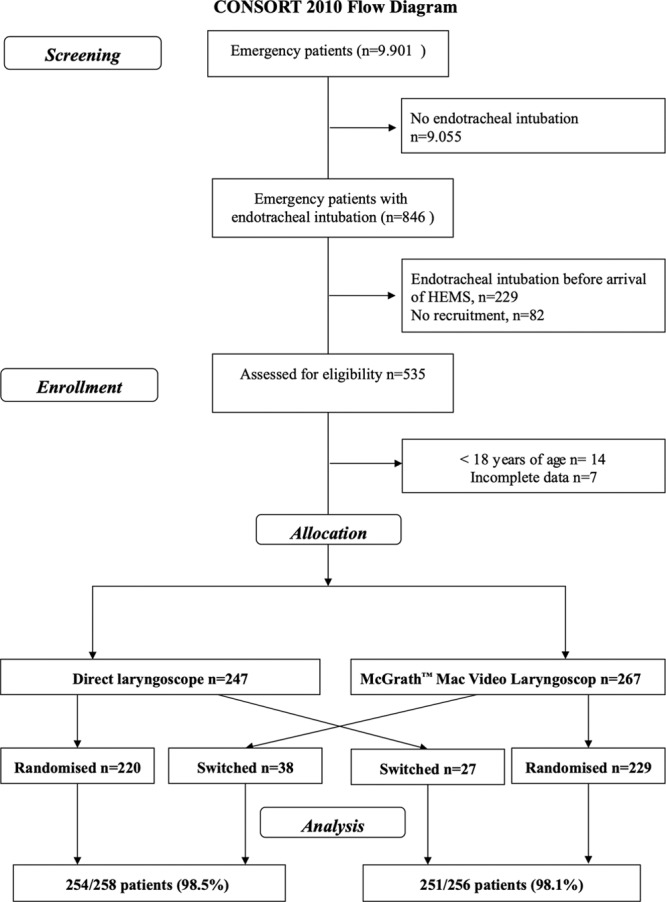
Patients: Five-hundred fourteen adult emergency patients (≥ 18 yr old).
Interventions: Helicopter Emergency Medical Service physicians followed the institutional algorithm, comprising a maximum of two tracheal intubation attempts with each device, followed by supraglottic, then surgical airway access in case of tracheal intubation failure. No restrictions were given for tracheal intubation indication.
Measurements main results: The Primary outcome was the rate of successful tracheal intubation; equivalence range was ± 6.5% of success rates. Secondary outcomes were the number of attempts to successful tracheal intubation, time to glottis passage and first end-tidal CO2 measurement, degree of glottis visualization, and number of problems. The success rate for the two devices was equivalent: direct laryngoscopy 98.5% (254/258), McGrath Mac Video Laryngoscope 98.1% (251/256) (difference, 0.4%; 99% CI, -2.58 to 3.39). There was no statistically significant difference with regard to tracheal intubation times, number of attempts or difficulty. The view to the glottis was significantly better, but the number of technical problems was increased with the McGrath Mac Video Laryngoscope. After a failed first tracheal intubation attempt, immediate switching of the device was significantly more successful than after the second attempt (90.5% vs 57.1%; p = 0.0003), regardless of the method.
Conclusions: Both devices are equivalently well suited for use in prehospital emergency tracheal intubation of adult patients. Switching the device following a failed first tracheal intubation attempt was more successful than a second attempt with the same device.
Conflict of interest statement
Dr. Trimmel disclosed that the study was funded in part by Oesterreichischer Automobil- und Touring Club, the motorist association of Austria (OEAMTC) Helicopter Emergency Medical Service (patient insurance fees). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Redundant Safety and Videolaryngoscopy.Crit Care Med. 2019 Oct;47(10):1462-1464. doi: 10.1097/CCM.0000000000003948. Crit Care Med. 2019. PMID: 31524699 No abstract available.
-
Videolaryngoscopy and Direct Laryngoscopy Equal for Air Medical Intubation? The Operator Matters.Crit Care Med. 2020 Mar;48(3):e254-e255. doi: 10.1097/CCM.0000000000004118. Crit Care Med. 2020. PMID: 32058397 No abstract available.
-
The authors reply.Crit Care Med. 2020 Mar;48(3):e255-e256. doi: 10.1097/CCM.0000000000004188. Crit Care Med. 2020. PMID: 32058398 No abstract available.
References
-
- Soar J, Nolan JP, Böttiger BW, et al. ; Adult advanced life support section Collaborators: European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015; 95:100–147 - PubMed
-
- Wang HE, Kupas DF, Hostler D, et al. Procedural experience with out-of-hospital endotracheal intubation. Crit Care Med 2005; 33:1718–1721 - PubMed
-
- Breckwoldt J, Klemstein S, Brunne B, et al. Difficult prehospital endotracheal intubation - predisposing factors in a physician based EMS. Resuscitation 2011; 82:1519–1524 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
