

Is Spinal Anesthesia Safer than General Anesthesia for Patients Undergoing Revision THA? Analysis of the ACS-NSQIP Database
- PMID: 31389887
- PMCID: PMC7000063
- DOI: 10.1097/CORR.0000000000000887
Is Spinal Anesthesia Safer than General Anesthesia for Patients Undergoing Revision THA? Analysis of the ACS-NSQIP Database
Abstract
Background: The incidence of revision THA continues to increase and there is a need to identify risk factors contributing to postoperative complications. Anesthesia type has been shown to be associated with complication rates in patients who undergo primary THA, but it is not clear whether the same is true among patients undergoing revision THA.
Questions/purposes: (1) After controlling for confounding variables, in the setting of a large-database analysis, is spinal anesthesia associated with a lower risk of death, readmission, reoperation, postoperative transfusion, thromboembolic events, surgical site infection (SSI), and re-intubation among patients undergoing revision THA?
Methods: The American College of Surgeons-National Surgical Quality Improvement (ACS-NSQIP) database was queried for patients undergoing aseptic, revision THA with either spinal or general anesthesia. Coarsened exact matching was used to match patients based on several baseline characteristics, including age, sex, body mass index, surgery type (Current Procedural Terminology code), and the modified Frailty Index score. Coarsened exact matching is a statistical method of exact matching that matches on chosen characteristics, in which continuous variables may be temporarily coarsened (such as, into discrete categorical variables) to facilitate matching. This method is an alternate to and requires less estimation than traditional propensity score matching. Then, using a model controlling for baseline patient characteristics and operative time, we performed multivariate logistic and linear regression analyses of matched cohorts to examine differences in mortality, readmission, reoperation, thromboembolic events, transfusion, SSI, and re-intubation.
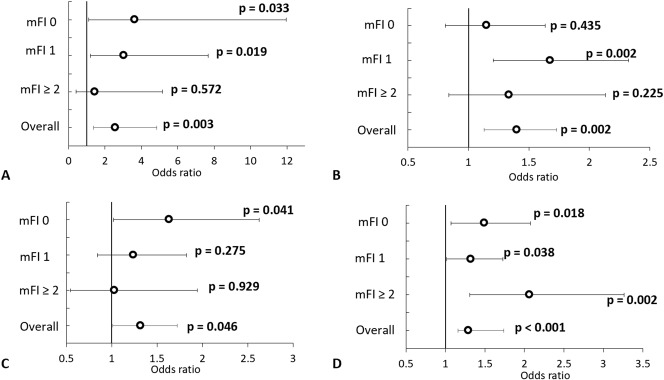
Results: After statistical matching and controlling for baseline demographic variables, surgery type (one- or two-component revision), surgical time and modified Frailty Index we found that patients receiving general anesthesia had higher odds of mortality (OR 3.72 [95% CI 1.31 to 10.50]; p = 0.013), readmission (OR 1.49 [95% CI 1.24 to 1.80]; p < 0.001), reoperation (OR 1.40 [95% CI 1.13 to 1.73]; p = 0.002), thromboembolic events (OR 2.57 [95% CI 1.37 to 4.84]; p = 0.003), SSI (OR 1.32 [95% CI 1.01 to 1.72]; p = 0.046), postoperative transfusion (OR 1.57 [95%CI 1.39 to 1.78]; p < 0.001) and unplanned intubation or failure to wean off intubation (OR 5.95 [95% CI 1.43 to 24.72]; p = 0.014).
Conclusions: In patients undergoing revision THA, spinal anesthesia is associated with a decreased risk of several complications. The current investigation suggests that, when practical (such as when long surgical times or changes to the surgical plan are not anticipated), spinal anesthesia should be considered for use during revision THA.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Is Spinal Anesthesia Safer than General Anesthesia for Patients Undergoing Revision THA? Analysis of the ACS-NSQIP Database.Clin Orthop Relat Res. 2020 Jan;478(1):88-89. doi: 10.1097/CORR.0000000000000937. Clin Orthop Relat Res. 2020. PMID: 31498262 Free PMC article. No abstract available.
Similar articles
-
General vs Spinal Anesthesia for Revision Total Knee Arthroplasty: Do Complication Rates Differ?J Arthroplasty. 2019 Jul;34(7):1417-1422. doi: 10.1016/j.arth.2019.03.048. Epub 2019 Mar 28. J Arthroplasty. 2019. PMID: 31005435
-
Are Patients Who Undergo THA for Infection at Higher Risk for 30-day Complications?Clin Orthop Relat Res. 2019 Jul;477(7):1624-1631. doi: 10.1097/CORR.0000000000000760. Clin Orthop Relat Res. 2019. PMID: 31268424 Free PMC article.
-
Is Obesity Associated With Increased Risk of Deep Vein Thrombosis or Pulmonary Embolism After Hip and Knee Arthroplasty? A Large Database Study.Clin Orthop Relat Res. 2019 Mar;477(3):523-532. doi: 10.1097/CORR.0000000000000615. Clin Orthop Relat Res. 2019. PMID: 30624321 Free PMC article.
-
Sex-specific differences in 30-day outcomes following primary total hip replacement in 86,684 patients.Hip Int. 2023 Sep;33(5):828-832. doi: 10.1177/11207000221110786. Epub 2022 Jul 14. Hip Int. 2023. PMID: 35836327 Review.
-
General anesthesia vs spinal anesthesia for patients undergoing total-hip arthroplasty: A meta-analysis.Medicine (Baltimore). 2019 Apr;98(16):e14925. doi: 10.1097/MD.0000000000014925. Medicine (Baltimore). 2019. PMID: 31008923 Free PMC article.
Cited by
-
Prevention of early complications following total hip replacement.SICOT J. 2021;7:61. doi: 10.1051/sicotj/2021060. Epub 2021 Nov 30. SICOT J. 2021. PMID: 34851264 Free PMC article.
-
The Prophylaxis Effect of Ephedrine on Hemodynamic Variation in Patients Undergoing Percutaneous Nephrolithotomy Surgery with Spinal Anesthesia.Int J Clin Pract. 2023 Feb 24;2023:8966501. doi: 10.1155/2023/8966501. eCollection 2023. Int J Clin Pract. 2023. PMID: 36874385 Free PMC article. Clinical Trial.
-
Outcomes following outpatient anterior cervical discectomy and fusion for the treatment of myelopathy.J Clin Orthop Trauma. 2020 Aug 9;15:161-167. doi: 10.1016/j.jcot.2020.07.030. eCollection 2021 Apr. J Clin Orthop Trauma. 2020. PMID: 33717932 Free PMC article.
-
Spinal Versus General Anesthesia in Contemporary Revision Total Knee Arthroplasties.J Arthroplasty. 2023 Jun;38(6S):S271-S274.e1. doi: 10.1016/j.arth.2023.01.053. Epub 2023 Feb 10. J Arthroplasty. 2023. PMID: 36773661 Free PMC article.
-
Delivering Essential Surgical Care for Lower-limb Musculoskeletal disorders in the Low-Resource Setting.World J Surg. 2021 Oct;45(10):2975-2981. doi: 10.1007/s00268-021-06211-3. Epub 2021 Jun 29. World J Surg. 2021. PMID: 34189619 Free PMC article.
References
-
- American College of Surgeons. User Guide for the 2015 ACS NSQIP Participant Use File (PUF). https://www.facs.org/∼/media/files/quality%20programs/nsqip/nsqip_puf_us.... Accessed May 20, 2016.
-
- Basques BA, Bohl DD, Golinvaux NS, Samuel AM, Grauer JG. General versus spinal anaesthesia for patients aged 70 years and older with a fracture of the hip. Bone Joint J. 2015;97-B:689-695. - PubMed
-
- Bellamy JL, Runner RP, Vu CCL, Schenker ML, Bradbury TL, Roberson JR. Modified Frailty Index is an effective risk assessment tool in primary total hip arthroplasty. J Arthroplasty. 2017;32:2963-2968. - PubMed
-
- Bohl DD, Singh K, Grauer JN. Nationwide databases in orthopaedic surgery research. J Am Acad Orthop Surg. 2016;24:673-682. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
