

Has a Prescription-limiting Law in Rhode Island Helped to Reduce Opioid Use After Total Joint Arthroplasty?
- PMID: 31389888
- PMCID: PMC7438153
- DOI: 10.1097/CORR.0000000000000885
Has a Prescription-limiting Law in Rhode Island Helped to Reduce Opioid Use After Total Joint Arthroplasty?
Abstract
Background: In the United States, since 2016, at least 28 of 50 state legislatures have passed laws regarding mandatory prescribing limits for opioid medications. One of the earliest state laws (which was passed in Rhode Island in 2016) restricted the maximum morphine milligram equivalents provided in the first postoperative prescription for patients defined as opioid-naïve to 30 morphine milligram equivalents per day, 150 total morphine milligram equivalents, or 20 total doses. While such regulations are increasingly common in the United States, their effects on opioid use after total joint arthroplasty are unclear.
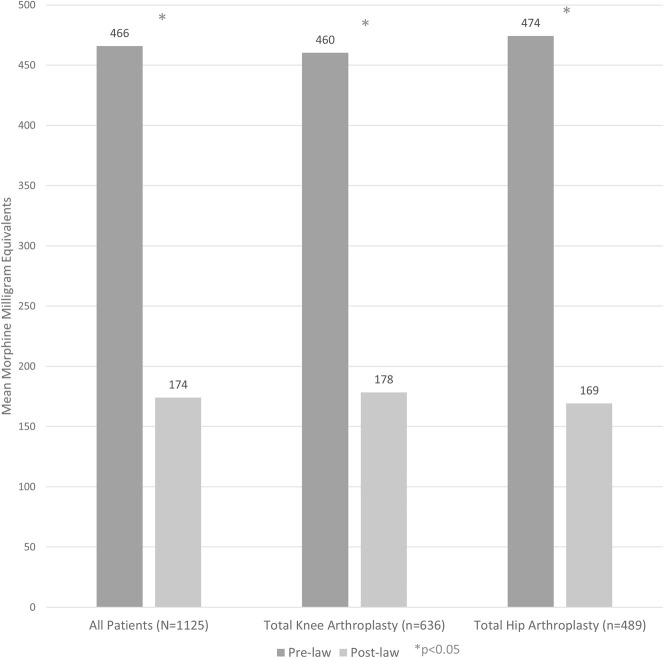
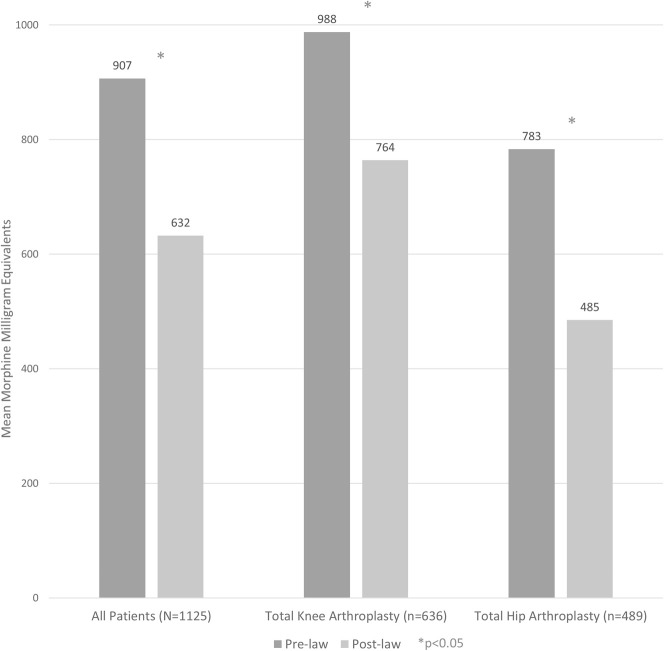
Questions/purposes: (1) Are legislative limitations to opioid prescriptions in Rhode Island associated with decreased opioid use in the immediate (first outpatient prescription postoperatively), 30-day, and 90-day periods after THA and TKA? (2) Is this law associated with similar changes in postoperative opioid use among patients who are opioid-naïve and those who are opioid-tolerant preoperatively?
Methods: Patients undergoing primary THA or TKA between January 1, 2016 and June 28, 2016 (before the law was passed on June 28, 2016) were retrospectively compared with patients undergoing surgery between June 1, 2017 and December 31, 2017 (after the law's implementation on April 17, 2017). The lapse between the pre-law and post-law periods was designed to avoid confounding from potential voluntary practice changes by physicians after the law was passed but before its mandatory implementation. Demographic and surgical details were extracted from a large multi-specialty orthopaedic group's surgical billing database using Current Procedural Terminology codes 27130 and 27447. Any patients undergoing revision procedures, same-day bilateral arthroplasties, or a second primary THA or TKA in the 3-month followup period were excluded. Secondary data were confirmed by reviewing individual electronic medical records in the associated hospital system which included three major hospital sites. We evaluated 1125 patients. In accordance with the state's department of health guidelines, patients were defined as opioid-tolerant if they had filled any prescription for an opioid medication in the 30-day preoperative period. Data on age, gender, and the proportion of patients who were defined as opioid tolerant preoperatively were collected and found to be no different between the pre-law and post-law groups. The state's prescription drug monitoring program database was used to collect data on prescriptions for all controlled substances filled between 30 days preoperatively and 90 days postoperatively. The primary outcomes were the mean morphine milligram equivalents of the initial outpatient postoperative opioid prescription after discharge and the mean cumulative morphine milligram equivalents at the 30- and 90-day postoperative intervals. Secondary analyses included subgroup analyses by procedure and by preoperative opioid tolerance.
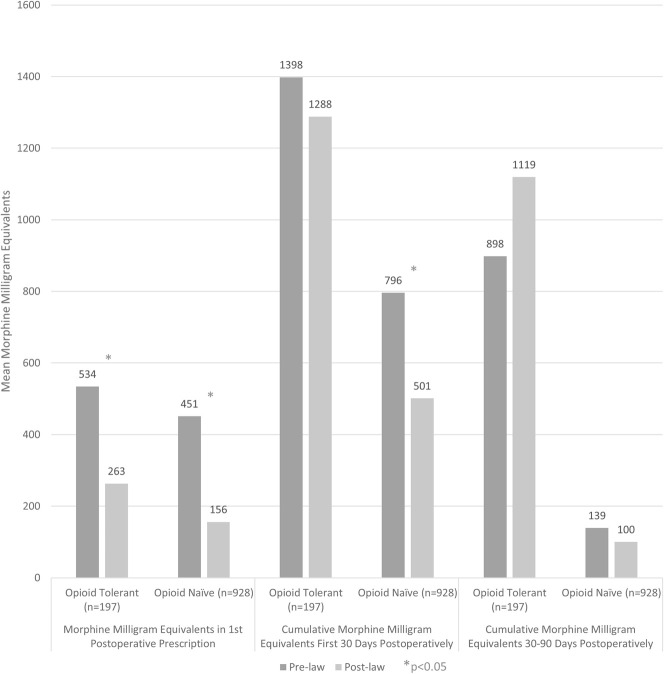
Results: After the law was implemented, the first opioid prescriptions were smaller for patients who were opioid-naïve (mean 156 ± 106 morphine milligram equivalents after the law's passage versus 451 ± 296 before, mean difference 294 morphine milligram equivalents; p < 0.001) and those who were opioid-tolerant (263 ± 265 morphine milligram equivalents after the law's passage versus 534 ± 427 before, mean difference 271 morphine milligram equivalents; p < 0.001); however, for cumulative prescriptions in the first 30 days postoperatively, this was only true among patients who were previously opioid-naïve (501 ± 416 morphine milligram equivalents after the law's passage versus 796 ± 597 before, mean difference 295 morphine milligram equivalents; p < 0.001). Those who were opioid-tolerant did not have a decrease in the cumulative number of 30-day morphine milligram equivalents (1288 ± 1632 morphine milligram equivalents after the law's passage versus 1398 ± 1274 before, mean difference 110 morphine milligram equivalents; p = 0.066).
Conclusions: The prescription-limiting law was associated with a decline in cumulative opioid prescriptions at 30 days postoperatively filled by patients who were opioid-naïve before total joint arthroplasty. This may substantially impact public health, and these policies should be considered an important tool for healthcare providers, communities, and policymakers who wish to combat the current opioid epidemic. However, given the lack of a discernible effect on cumulative opioids filled from 30 to 90 days postoperatively, further investigations are needed to evaluate more effective policies to prevent prolonged opioid use after total joint arthroplasty, particularly in patients who are opioid-tolerant preoperatively.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
Each author certifies that neither he, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment on
-
Editor's Spotlight/Take 5: Has Prescription-limiting Legislation in Rhode Island Helped to Reduce Opioid Use After Total Joint Arthroplasty?Clin Orthop Relat Res. 2020 Feb;478(2):200-204. doi: 10.1097/CORR.0000000000001109. Clin Orthop Relat Res. 2020. PMID: 31899743 Free PMC article. No abstract available.
Similar articles
-
Mandatory Prescription Limits and Opioid Utilization Following Orthopaedic Surgery.J Bone Joint Surg Am. 2019 May 15;101(10):e43. doi: 10.2106/JBJS.18.00943. J Bone Joint Surg Am. 2019. PMID: 31094987
-
Effect of narcotic prescription limiting legislation on opioid utilization following lumbar spine surgery.Spine J. 2019 Apr;19(4):717-725. doi: 10.1016/j.spinee.2018.09.007. Epub 2018 Sep 14. Spine J. 2019. PMID: 30223089
-
What Changes Have Occurred in Opioid Prescriptions and the Prescribers of Opioids Before TKA and THA? A Large National Registry Study.Clin Orthop Relat Res. 2023 Sep 1;481(9):1716-1728. doi: 10.1097/CORR.0000000000002653. Epub 2023 Apr 26. Clin Orthop Relat Res. 2023. PMID: 37099415 Free PMC article.
-
National and State Level Opioid-Restricting Legislation in Total Joint Arthroplasty: A Systematic Review.J Arthroplasty. 2022 Jan;37(1):176-185. doi: 10.1016/j.arth.2021.07.013. Epub 2021 Jul 31. J Arthroplasty. 2022. PMID: 34456092
-
Postoperative Opioid Consumption is Greater after Simultaneous versus Staged Bilateral Total Knee Arthroplasty.J Knee Surg. 2024 May;37(6):436-443. doi: 10.1055/s-0043-1775872. Epub 2023 Oct 18. J Knee Surg. 2024. PMID: 37852291 Review.
Cited by
-
Editor's Spotlight/Take 5: What Is the Financial Impact of Orthopaedic Sequelae of Intravenous Drug Use on Urban Tertiary-care Centers?Clin Orthop Relat Res. 2020 Oct;478(10):2197-2201. doi: 10.1097/CORR.0000000000001474. Clin Orthop Relat Res. 2020. PMID: 32898040 Free PMC article. No abstract available.
-
Editor's Spotlight/Take 5: Has Prescription-limiting Legislation in Rhode Island Helped to Reduce Opioid Use After Total Joint Arthroplasty?Clin Orthop Relat Res. 2020 Feb;478(2):200-204. doi: 10.1097/CORR.0000000000001109. Clin Orthop Relat Res. 2020. PMID: 31899743 Free PMC article. No abstract available.
-
Post-lumbar surgery prescription variation and opioid-related outcomes in a large US healthcare system: an observational study.Spine J. 2023 Sep;23(9):1345-1357. doi: 10.1016/j.spinee.2023.05.006. Epub 2023 May 22. Spine J. 2023. PMID: 37220814 Free PMC article.
-
Strategies aimed at preventing long-term opioid use in trauma and orthopaedic surgery: a scoping review.BMC Musculoskelet Disord. 2022 Mar 11;23(1):238. doi: 10.1186/s12891-022-05044-y. BMC Musculoskelet Disord. 2022. PMID: 35277150 Free PMC article.
-
Narcotic Refills and Patient Satisfaction With Pain Control After Total Joint Arthroplasty.J Arthroplasty. 2021 Feb;36(2):454-461. doi: 10.1016/j.arth.2020.07.073. Epub 2020 Aug 4. J Arthroplasty. 2021. PMID: 32839063 Free PMC article.
References
-
- American Academy of Orthopaedic Surgeons. Opioid use, misuse, and abuse in orthopaedic practice. Available at: https://www.aaos.org/uploadedfiles/preproduction/about/opinion_statement.... Accessed September 11, 2018.
-
- Archambault S, Lombardi F, Prata E, McCaffrey M, Metts H. Chapter 21-28 Uniform Controlled Substances Act. Available at: http://webserver.rilin.state.ri.us/Statutes/TITLE21/21-28/INDEX.HTM. Accessed March 29, 2019.
-
- Bedard NA, DeMik DE, Dowdle SB, Owens JM, Liu SS, Callaghan JJ. Preoperative opioid use and its association with early revision of total knee arthroplasty. J Arthroplasty. 2018;33:3520-3523. - PubMed
-
- Bedard NA, Pugely AJ, Westermann RW, Duchman KR, Glass NA, Callaghan JJ. Opioid use after total knee arthroplasty: trends and risk factors for prolonged use. J Arthroplasty. 2017;32:2390-2394. - PubMed
-
- Bicket M, White E, Wu C, Pronovost P, Yaster M, Alexander G. (232) Prescription opioid oversupply following orthopedic surgery: a prospective cohort study. J Pain. 2017;18:S34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
