

Comparison of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy With Systematic Biopsy Alone for the Diagnosis of Prostate Cancer: A Systematic Review and Meta-analysis
- PMID: 31390032
- PMCID: PMC6686781
- DOI: 10.1001/jamanetworkopen.2019.8427
Comparison of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy With Systematic Biopsy Alone for the Diagnosis of Prostate Cancer: A Systematic Review and Meta-analysis
Abstract
Importance: The current diagnostic pathway for patients with suspected prostate cancer (PCa) includes prostate biopsy. A large proportion of individuals who undergo biopsy have either no PCa or low-risk disease that does not require treatment. Unnecessary biopsies may potentially be avoided with prebiopsy imaging.
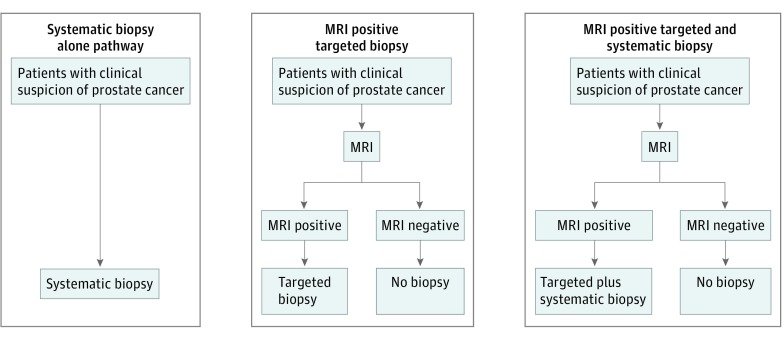
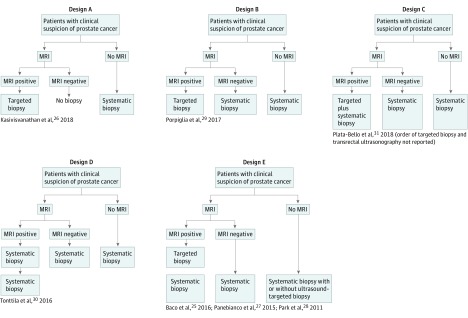
Objective: To compare the performance of systematic transrectal ultrasonography-guided prostate biopsy vs prebiopsy biparametric or multiparametric magnetic resonance imaging (MRI) followed by targeted biopsy with or without systematic biopsy.
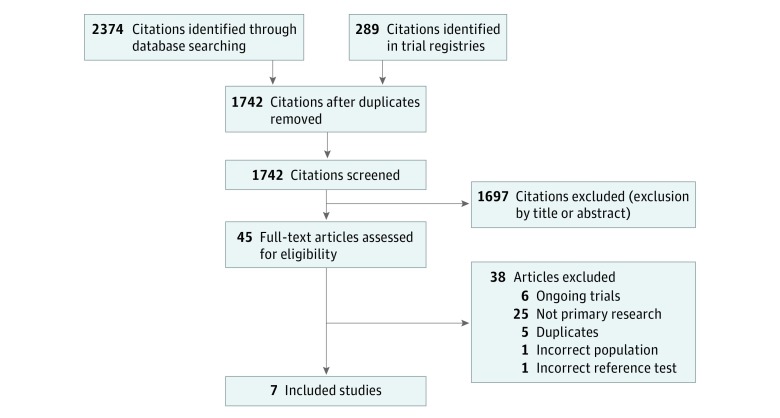
Data sources: MEDLINE, Embase, Cochrane, Web of Science, clinical trial registries, and reference lists of recent reviews were searched through December 2018 for randomized clinical trials using the terms "prostate cancer" and "MRI."
Study selection: Randomized clinical trials comparing diagnostic pathways including prebiopsy MRI vs systematic transrectal ultrasonography-guided biopsy in biopsy-naive men with a clinical suspicion of PCa.
Data extraction and synthesis: Data were pooled using random-effects meta-analysis. Risk of bias was assessed using the revised Cochrane tool. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed. All review stages were conducted by 2 reviewers.
Main outcomes and measures: Detection rate of clinically significant and insignificant PCa, number of biopsy procedures, number of biopsy cores taken, and complications.
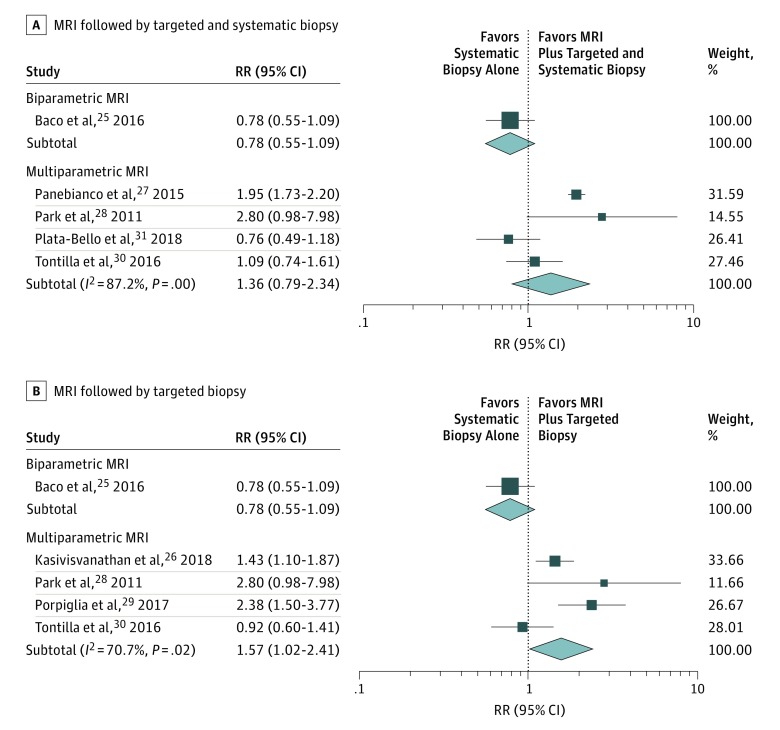
Results: Seven high-quality trials (2582 patients) were included. Compared with systematic transrectal ultrasonography-guided biopsy alone, MRI with or without targeted biopsy was associated with a 57% (95% CI, 2%-141%) improvement in the detection of clinically significant PCa, a 33% (95% CI, 23%-45%) potential reduction in the number of biopsy procedures, and a 77% (95% CI, 60%-93%) reduction in the number of cores taken per procedure. One trial showed reduced pain and bleeding adverse effects. Systematic sampling of the prostate in addition to the acquisition of targeted cores did not significantly improve the detection of clinically significant PCa compared with systematic biopsy alone.
Conclusions and relevance: In this meta-analysis, prebiopsy MRI combined with targeted biopsy vs systematic transrectal ultrasonography-guided biopsy alone was associated with improved detection of clinically significant PCa, despite substantial heterogeneity among trials. Prebiopsy MRI was associated with a reduced number of individual biopsy cores taken per procedure and with reduced adverse effects, and it potentially prevented unnecessary biopsies in some individuals. This evidence supports implementation of prebiopsy MRI into diagnostic pathways for suspected PCa.
Conflict of interest statement
Figures
Comment in
-
The Evolving Paradigm of Prostate Cancer Screening.JAMA Netw Open. 2019 Aug 2;2(8):e198392. doi: 10.1001/jamanetworkopen.2019.8392. JAMA Netw Open. 2019. PMID: 31390029 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
