Effect of Telephone-Delivered Collaborative Goal Setting and Behavioral Activation vs Enhanced Usual Care for Depression Among Adults With Uncontrolled Diabetes: A Randomized Clinical Trial
- PMID: 31390035
- PMCID: PMC6686779
- DOI: 10.1001/jamanetworkopen.2019.8634
Effect of Telephone-Delivered Collaborative Goal Setting and Behavioral Activation vs Enhanced Usual Care for Depression Among Adults With Uncontrolled Diabetes: A Randomized Clinical Trial
Abstract
Importance: Depression symptoms are present in one-third of patients with diabetes, contributing to significant adverse consequences. Population screening of high-risk patients coupled with telephone delivery of evidence-based therapies for comorbid diabetes may address barriers to care.
Objective: To evaluate the effectiveness of proactive population screening plus telephone delivery of a collaborative goal-setting intervention among high-risk patients with uncontrolled diabetes and depression.
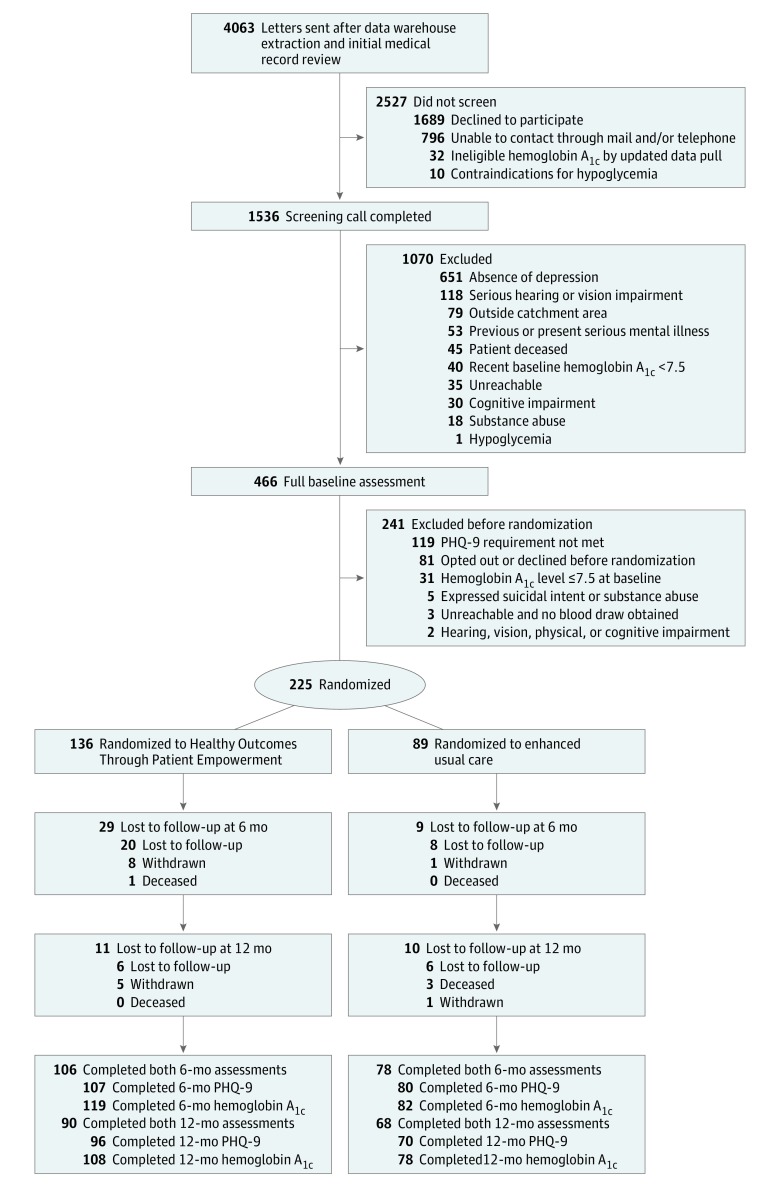
Design, setting, and participants: In this randomized clinical trial, 225 participants (intervention [n = 136] and control [n = 89]) were enrolled from a regional Veterans Healthcare System serving Southeast Texas from November 1, 2012, through June 24, 2016. Data were gathered at baseline and 6 and 12 months after intervention. Patients selected had uncontrolled diabetes (hemoglobin A1c [HbA1c] >7.5%]) and clinically significant depression (Patient Health Questionnaire-9 scores [PHQ-9] ≥10) and were living more than 20 miles from the Veterans Affairs medical center. Data collection was completed on December 6, 2016, and final analyses were completed by January 25, 2018. All analyses were intent to treat.
Interventions: Healthy Outcomes Through Patient Empowerment (HOPE) included 9 telephone sessions with 24 trained health care professionals using collaborative goal-setting and behavioral activation methods. The control group received enhanced usual care (EUC) and notification of high-risk status.
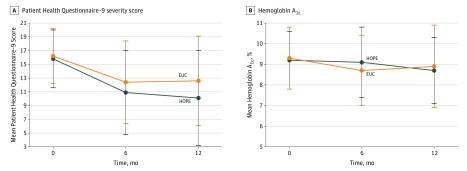
Main outcomes and measures: Change in depression symptoms using PHQ-9 and glycemic control using HbA1c from baseline to 6 months and to 12 months. Secondary analyses evaluated clinically significant responses for these measures.
Results: Among 225 participants, 202 (89.8%) were men, the mean (SD) age was 61.9 (8.3) years, 145 (64.4%) were married, and 156 (69.3%) had some education beyond high school. For the overall study, 38 participants (16.9%) were lost to follow-up or withdrew at 6 months and another 21 (9.3%) were lost to follow-up or withdrew at 12 months. Repeated-measures analysis with multiple imputation for missing data assessing the interaction of treatment group (HOPE vs EUC) and time (baseline, 6 months, and 12 months) found no significant improvement in PHQ-9 (β, 1.56; 95% CI, -0.68 to 3.81; P = .17) or HbA1c (β, -0.005; 95% CI, -0.73 to 0.72; P = .82). Analyses using t test for change from baseline to 12 months showed a HOPE vs EUC between-group mean difference for PHQ-9 of 2.14 (95% CI, 0.18 to 4.10; P = .03) and for HbA1c of -0.06% (95% CI, -0.61% to 0.50%; P = .83). A secondary analysis of patients experiencing a clinical response found that 52.1% of HOPE participants had clinically significant responses in PHQ-9 at 12 months vs 32.9% in EUC (difference, 0.19; 95% CI, 0.04-0.33; P = .01).
Conclusions and relevance: Telephone-delivered, collaborative goal setting produced clinically significant reductions in depression symptoms but not glycemic control among patients who remained engaged at 12 months compared with EUC among a population screened sample of high-risk patients with diabetes and depression. Although the intervention created some lasting effect for depression, additional strategies are needed to maintain engagement of this high-risk population within an interprofessional team approach to primary care.
Trial registration: ClinicalTrials.gov identifier: NCT01572389.
Conflict of interest statement
Figures