

Long-term Host Immune Response Trajectories Among Hospitalized Patients With Sepsis
- PMID: 31390038
- PMCID: PMC6686981
- DOI: 10.1001/jamanetworkopen.2019.8686
Long-term Host Immune Response Trajectories Among Hospitalized Patients With Sepsis
Abstract
Importance: Long-term immune sequelae after sepsis are poorly understood.
Objective: To assess whether abnormalities in the host immune response during hospitalization for sepsis persist after discharge.
Design, settings, and participants: This prospective, multicenter cohort study enrolled and followed up for 1 year adults who survived a hospitalization for sepsis from January 10, 2012, to May 25, 2017, at 12 US hospitals.
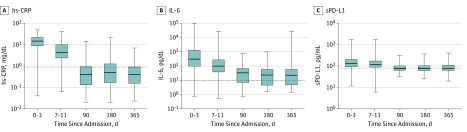
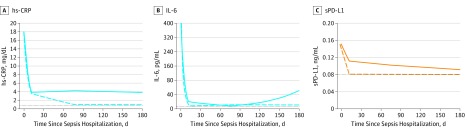
Exposures: Circulating levels of inflammation (interleukin 6 and high-sensitivity C-reactive protein [hs-CRP]), immunosuppression (soluble programmed death ligand 1 [sPD-L1]), hemostasis (plasminogen activator inhibitor 1 and D-dimer), endothelial dysfunction (E-selectin, intercellular adhesion molecule 1, and vascular cell adhesion molecule 1), and oxidative stress biomarkers were measured at 5 time points during and after hospitalization for sepsis for 1 year. Individual biomarker trajectories and patterns of trajectories across biomarkers (phenotypes) were identified.
Main outcomes and measures: Outcomes were adjudicated centrally and included all-cause and cause-specific readmissions and mortality.
Results: A total of 483 patients (mean [SD] age, 60.5 [15.2] years; 265 [54.9%] male) who survived hospitalization for sepsis were included in the study. A total of 376 patients (77.8%) had at least 1 chronic disease, and their mean (SD) Sequential Organ Failure Assessment score was 4.2 (3.0). Readmissions were common (485 readmissions in 205 patients [42.5%]), and 43 patients (8.9%) died by 3 months, 56 patients (11.6%) died by 6 months, and 85 patients (17.6%) died by 12 months. Elevated hs-CRP levels were observed in 23 patients (25.8%) at 3 months, 26 patients (30.2%) at 6 months, and 23 patients (25.6%) at 12 months, and elevated sPD-L1 levels were observed in 45 patients (46.4%) at 3 months, 40 patients (44.9%) at 6 months, and 44 patients (49.4%) at 12 months. Two common phenotypes were identified based on hs-CRP and sPDL1 trajectories: high hs-CRP and sPDL1 levels (hyperinflammation and immunosuppression phenotype [326 of 477 (68.3%)]) and normal hs-CRP and sPDL1 levels (normal phenotype [143 of 477 (30.0%)]). These phenotypes had similar clinical characteristics and clinical course during hospitalization for sepsis. Compared with normal phenotype, those with the hyperinflammation and immunosuppression phenotype had higher 1-year mortality (odds ratio, 8.26; 95% CI, 3.45-21.69; P < .001), 6-month all-cause readmission or mortality (hazard ratio [HR], 1.53; 95% CI, 1.10-2.13; P = .01), and 6-month readmission or mortality attributable to cardiovascular disease (HR, 5.07; 95% CI, 1.18-21.84; P = .02) or cancer (HR, 5.15; 95% CI, 1.25-21.18; P = .02). These associations were adjusted for demographic characteristics, chronic diseases, illness severity, organ support, and infection site during sepsis hospitalization and were robust in sensitivity analyses.
Conclusions and relevance: In this study, persistent elevation of inflammation and immunosuppression biomarkers occurred in two-thirds of patients who survived a hospitalization for sepsis and was associated with worse long-term outcomes.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
