

Peripheral Nervous System Disease in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
- PMID: 31390162
- PMCID: PMC6935421
- DOI: 10.1002/art.41070
Peripheral Nervous System Disease in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
Abstract
Objective: To determine the frequency, clinical characteristics, associations, and outcomes of different types of peripheral nervous system (PNS) disease in a multiethnic/multiracial, prospective inception cohort of systemic lupus erythematosus (SLE) patients.
Methods: Patients were evaluated annually for 19 neuropsychiatric (NP) events including 7 types of PNS disease. SLE disease activity, organ damage, autoantibodies, and patient and physician assessment of outcome were measured. Time to event and linear regressions were used as appropriate.
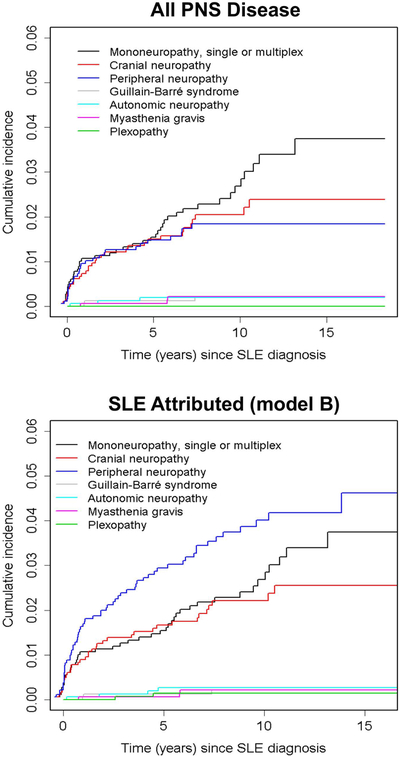
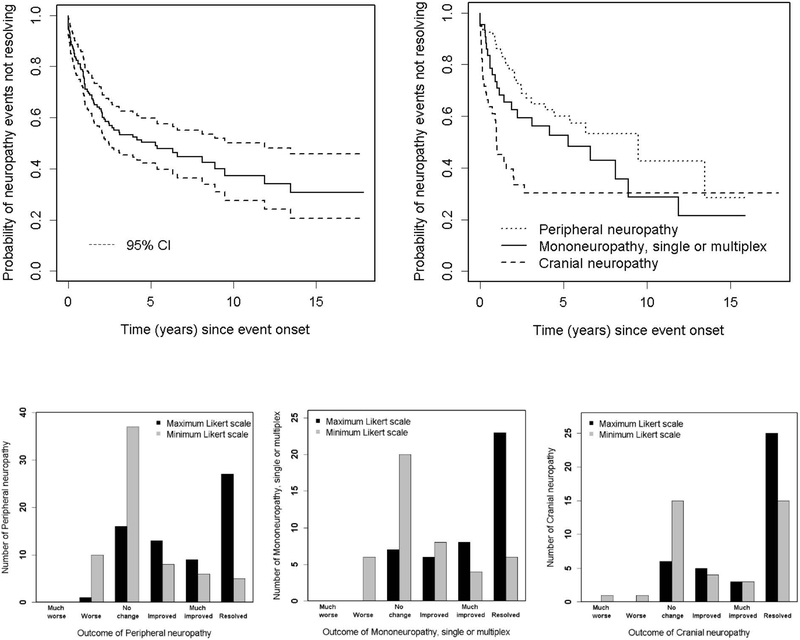
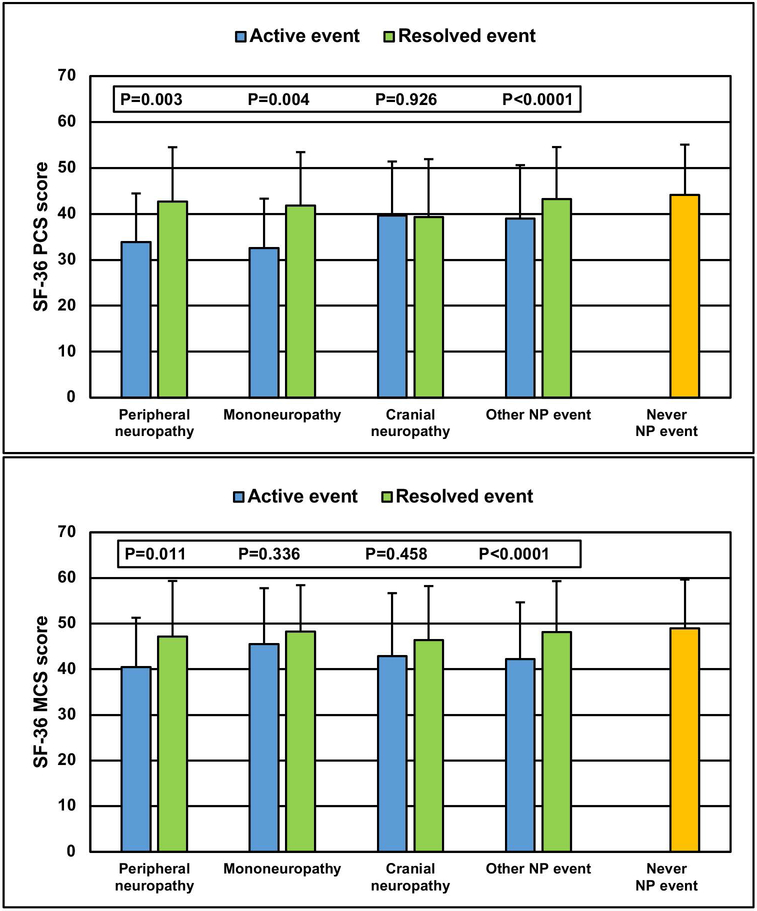
Results: Of 1,827 SLE patients, 88.8% were female, and 48.8% were white. The mean ± SD age was 35.1 ± 13.3 years, disease duration at enrollment was 5.6 ± 4.2 months, and follow-up was 7.6 ± 4.6 years. There were 161 PNS events in 139 (7.6%) of 1,827 patients. The predominant events were peripheral neuropathy (66 of 161 [41.0%]), mononeuropathy (44 of 161 [27.3%]), and cranial neuropathy (39 of 161 [24.2%]), and the majority were attributed to SLE. Multivariate Cox regressions suggested longer time to resolution in patients with a history of neuropathy, older age at SLE diagnosis, higher SLE Disease Activity Index 2000 scores, and for peripheral neuropathy versus other neuropathies. Neuropathy was associated with significantly lower Short Form 36 (SF-36) physical and mental component summary scores versus no NP events. According to physician assessment, the majority of neuropathies resolved or improved over time, which was associated with improvements in SF-36 summary scores for peripheral neuropathy and mononeuropathy.
Conclusion: PNS disease is an important component of total NPSLE and has a significant negative impact on health-related quality of life. The outcome is favorable for most patients, but our findings indicate that several factors are associated with longer time to resolution.
© 2019, American College of Rheumatology.
Figures

References
-
- Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. - PubMed
-
- The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999;42(4):599–608. - PubMed
Publication types
MeSH terms
Grants and funding
- M01 RR000046/RR/NCRR NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- DH_/Department of Health/United Kingdom
- UL1 RR025741/RR/NCRR NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- MC_UU_00002/11/MRC_/Medical Research Council/United Kingdom
- P30 AR072579/AR/NIAMS NIH HHS/United States
- MC_UU_00002/8/MRC_/Medical Research Council/United Kingdom
- R01 AR069572/AR/NIAMS NIH HHS/United States
- MC_U105261167/MRC_/Medical Research Council/United Kingdom
- P60 AR064464/AR/NIAMS NIH HHS/United States
- P60 AR048098/AR/NIAMS NIH HHS/United States
- R01 AR043727/AR/NIAMS NIH HHS/United States
- ARC_/Arthritis Research UK/United Kingdom
- K24 AR002138/AR/NIAMS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
