

Evolution of mitral regurgitation in patients with heart failure referred to a tertiary heart failure clinic
- PMID: 31390167
- PMCID: PMC6816234
- DOI: 10.1002/ehf2.12478
Evolution of mitral regurgitation in patients with heart failure referred to a tertiary heart failure clinic
Abstract
Aims: Significant mitral regurgitation (MR) is an important predictor for all-cause mortality and heart failure (HF) hospitalizations independent of left ventricular ejection fraction (LVEF). The aims of this study were to investigate (i) in how many patients referred to a tertiary outpatient HF clinic HF therapy could be optimized, (ii) the effect of optimized treatment on MR severity, and (iii) whether a reduction in MR resulted in improvement of symptoms.
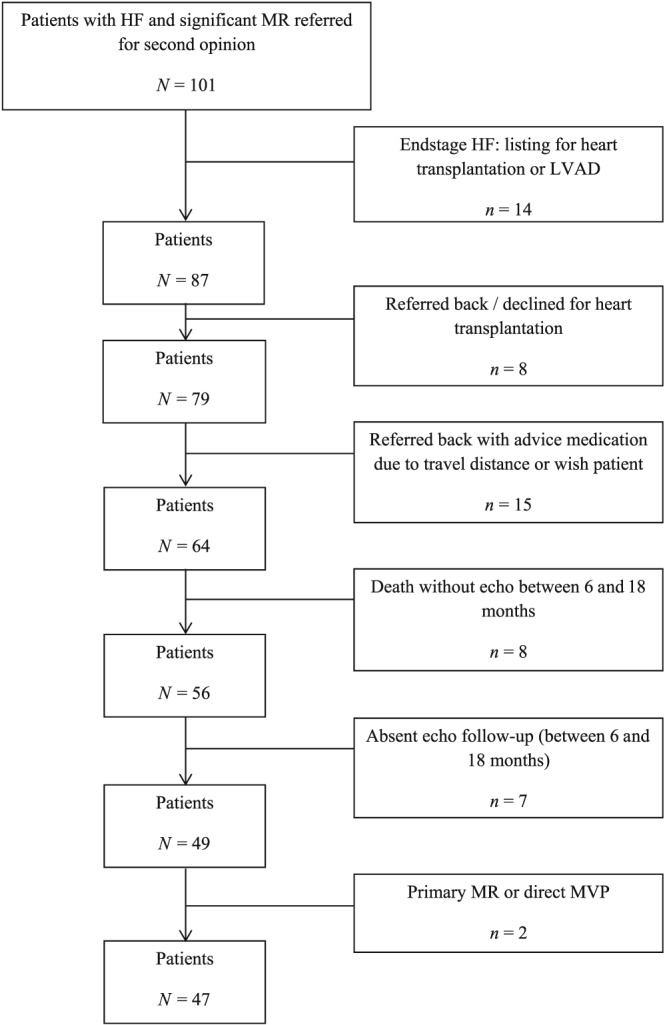
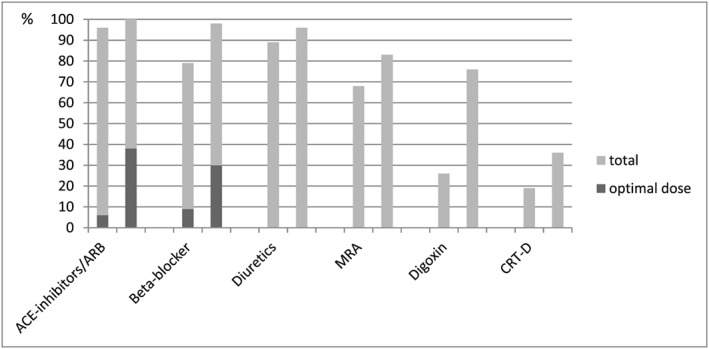
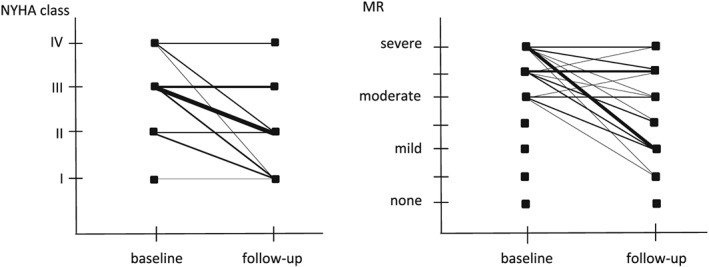
Methods and results: Forty-seven referred patients with therapy-resistant symptomatic chronic HF with an LVEF <40% and at least moderate MR were analysed on admission and after optimization of HF treatment after 6-18 months. The patients were classified as a volume responder when LV end-systolic volume (LVESV) decreased ≥15%, as LVEF responder when LVEF increased by ≥5% points, as clinical responder when New York Heart Association (NYHA) class improved at least one category, and as MR responder when MR severity improved at least one category to maximally moderate. After 14 ± 4 months of treatment optimization, optimal doses of angiotensin-converting enzyme inhibitors/angiotensin receptor blocker were seen in 18 (38%) patients compared with three (6%) at baseline (P < 0.001), and optimal doses of beta-blockers were seen in 14 (30%) patients compared with four (9%) at baseline (P < 0.001). In total, 68% of the patients were clinical responders, 57% MR responders, 34% volumetric responders, and 49% LVEF responders. NYHA class improved from 2.9 ± 0.6 to 2.0 ± 0.9 (P < 0.001), MR class from 5.2 ± 0.8 to 3.6 ± 1.5 (P < 0.001), LVEF from 24% ± 9% to 31% ± 12% (P < 0.01), and LVESV non-significantly improved. The positive predictive value of MR response to NYHA response was 88%; the negative predictive value was 53%, agreement 69%, and kappa 0.39. The positive predictive value of LVEF response to NYHA response was 76%; the negative predictive value was 44%, agreement 60%, and kappa 0.21. The positive predictive value of LVESV volume response to NYHA response was 75%; the negative predictive value was 39%, agreement 51%, and kappa 0.12.
Conclusions: Although this study was limited by a small number of patients, initiation and up-titration of recommended HF therapy in patients referred to our tertiary HF outpatient clinic resulted in significant MR reduction in over half of the patients, emphasizing the importance of optimal medical treatment in these very sick cardiac patients with otherwise grave prognosis. MR reduction was best correlated to NYHA improvement.
Keywords: Echocardiography; Heart failure; Mitral regurgitation.
Conflict of interest statement
None declared.
Figures
References
-
- Rossi A, Dini FL, Faggiano P, Agricola E, Cicoira M, Frattini S, Simioniuc A, Gullace M, Ghio S, Enriquez‐Sarano M, Temporelli PL. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non‐ischaemic dilated cardiomyopathy. Heart 2011; 97: 1675–1680. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. - PubMed
-
- Capomolla S, Febo O, Gnemmi M, Riccardi G, Opasich C, Caporotondi A, Mortara A, Pinna GD, Cobelli F. Beta‐blockade therapy in chronic heart failure: diastolic function and mitral regurgitation improvement by carvedilol. Am Heart J 2000; 139: 596–608. - PubMed
-
- Comin‐Colet J, Sanchez‐Corral MA, Manito N, Gomez‐Hospital JA, Roca J, Fernandez‐Nofrerias E, Valdovinos P, Esplugas E. Effect of carvedilol therapy on functional mitral regurgitation, ventricular remodeling, and contractility in patients with heart failure due to left ventricular systolic dysfunction. Transplant Proc 2002; 34: 177–178. - PubMed
-
- Lowes BD, Gill EA, Abraham WT, Larrain JR, Robertson AD, Bristow MR, Gilbert EM. Effects of carvedilol on left ventricular mass, chamber geometry, and mitral regurgitation in chronic heart failure. Am J Cardiol 1999; 83: 1201–1205. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
