

Refining the Association Between Body Mass Index and Atrial Fibrillation: G-Formula and Restricted Mean Survival Times
- PMID: 31390924
- PMCID: PMC6759878
- DOI: 10.1161/JAHA.119.013011
Refining the Association Between Body Mass Index and Atrial Fibrillation: G-Formula and Restricted Mean Survival Times
Abstract
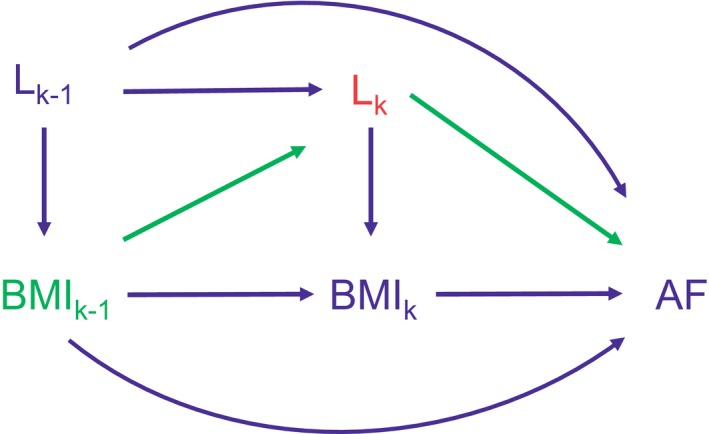
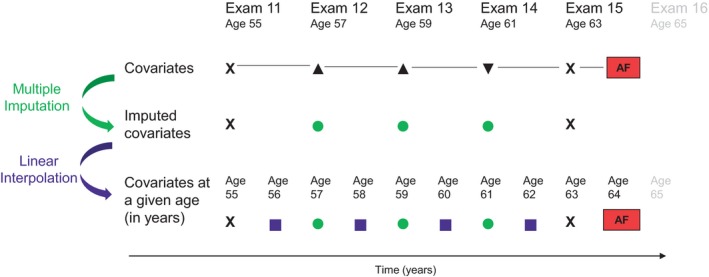
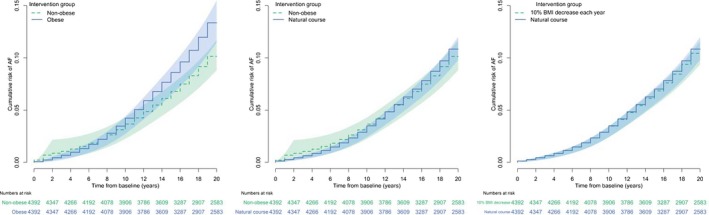
Background Previous studies assessing the association between body mass index (BMI) and atrial fibrillation (AF) did not account for time-varying covariates, which may be affected by previous BMI. We illustrate how the g-formula can account for time-varying confounding. Methods and Results We included 4392 participants from the Framingham Heart Study who were AF free at ages 45 to 55 years, and followed them for up to 20 years. We estimated hazard ratios (HRs) comparing time-varying nonobese versus obese with Cox models. We used the g-formula to compare nonobese versus obese and 10% annual decrease in BMI (until normal weight is reached) versus natural course. We estimated HRs and differences in restricted mean survival times, the mean difference in time alive and AF free. We adjusted for sex, age, and time-varying risk factors. Cox models indicated that nonobese participants had a decreased rate of AF versus obese participants (HR, 0.83; 95% CI, 0.72-0.97). G-formula analyses comparing everyone had they been nonobese versus obese yielded stronger associations (HR, 0.73; 95% CI, 0.58-0.91). The restricted mean survival time was 19.22 years had everyone been nonobese and 19.03 years had everyone been obese (difference, 2.25 months; 95% CI, -0.66 to 5.16). When assessing a 10% annual decrease in BMI, the association was weaker (HR 0.96; 95% CI, 0.86-1.08). Conclusions Decreased BMI was associated with a lower rate of AF after accounting for time-varying covariates that depend on previous exposure using the g-formula, which Cox models cannot accommodate. Absolute measures like the restricted mean survival time difference offer context to relative measures of association.
Keywords: atrial fibrillation; body mass index; epidemiology; survival analysis; time‐varying covariate.
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Benjamin EJ, Chen PS, Bild DE, Mascette AM, Albert CM, Alonso A, Calkins H, Connolly SJ, Curtis AB, Darbar D, Ellinor PT, Go AS, Goldschlager NF, Heckbert SR, Jalife J, Kerr CR, Levy D, Lloyd‐Jones DM, Massie BM, Nattel S, Olgin JE, Packer DL, Po SS, Tsang TS, Van Wagoner DR, Waldo AL, Wyse DG. Prevention of atrial fibrillation: report from a National Heart, Lung, and Blood Institute workshop. Circulation. 2009;119:606–618. - PMC - PubMed
-
- Alonso A, Krijthe BP, Aspelund T, Stepas KA, Pencina MJ, Moser CB, Sinner MF, Sotoodehnia N, Fontes JD, Janssens AC, Kronmal RA, Magnani JW, Witteman JC, Chamberlain AM, Lubitz SA, Schnabel RB, Agarwal SK, McManus DD, Ellinor PT, Larson MG, Burke GL, Launer LJ, Hofman A, Levy D, Gottdiener JS, Kaab S, Couper D, Harris TB, Soliman EZ, Stricker BH, Gudnason V, Heckbert SR, Benjamin EJ. Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: the CHARGE‐AF consortium. J Am Heart Assoc. 2013;2:e000102 DOI: 10.1161/JAHA.112.000102. - DOI - PMC - PubMed
-
- Berkovitch A, Kivity S, Klempfner R, Segev S, Milwidsky A, Erez A, Sabbag A, Goldenberg I, Sidi Y, Maor E. Body mass index and the risk of new‐onset atrial fibrillation in middle‐aged adults. Am Heart J. 2016;173:41–48. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
